Anomalous Left Circumflex PCI with Wire Knuckle Push Technique
by
Avin Pothuloori
April 2, 2012Operator(s)
Adam Stys, MD, FACC, FSCAI, FASA
Affiliation
University of South Dakota Sanford School of Medicine
Facility / Institute
Sanford USD Medical Center, Sioux Falls, SD, USA
Clinical History
A 56-year-old male - known severe anomalous left circumflex disease managed medically - presented with unstable angina pectoris. Past medical history was significant for hypertension, hyperlipidemia, and diabetes. Cardiovascular physical examination was unremarkable. EKG showed sinus bradycardia rhythm and diffuse, mild ST segment elevations. Echocardiogram showed normal left ventricular systolic function, normal valves, and no pericardial effusion. Troponin I level was initially normal. The patient was treated with IV heparin, nitroglycerin, beta blocker, statin and aspirin.
Angiography
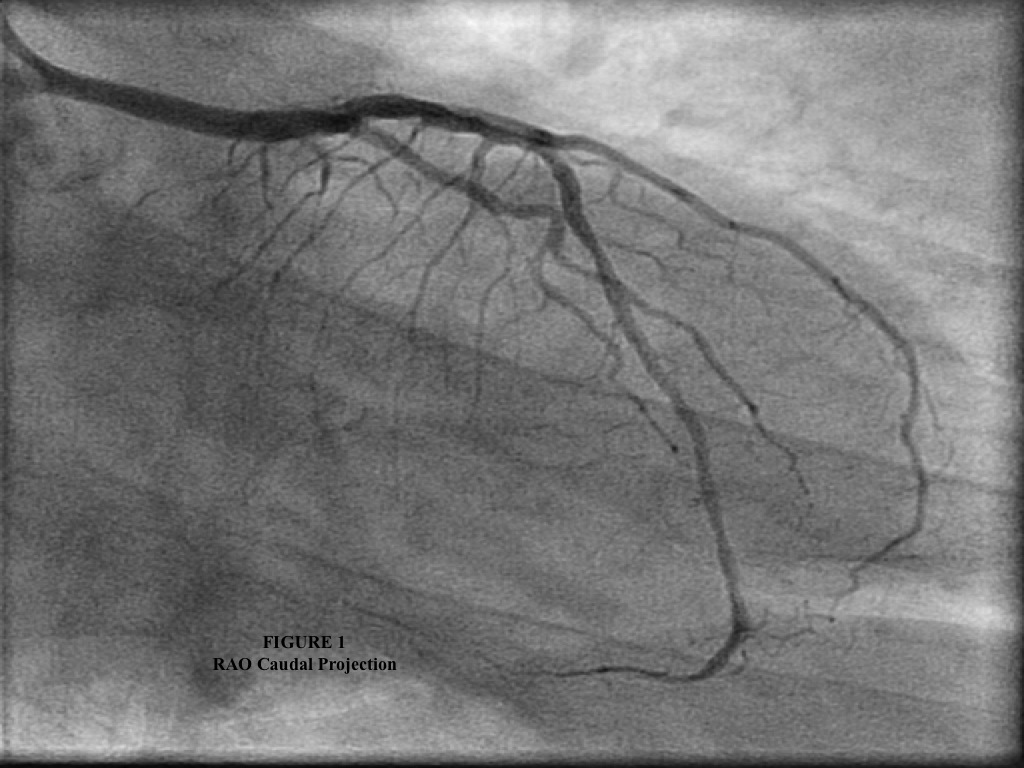
1. LAD had no obstructive disease; however left circumflex was not visualized on the left system injection (Figure 1 is RAO caudal projection).
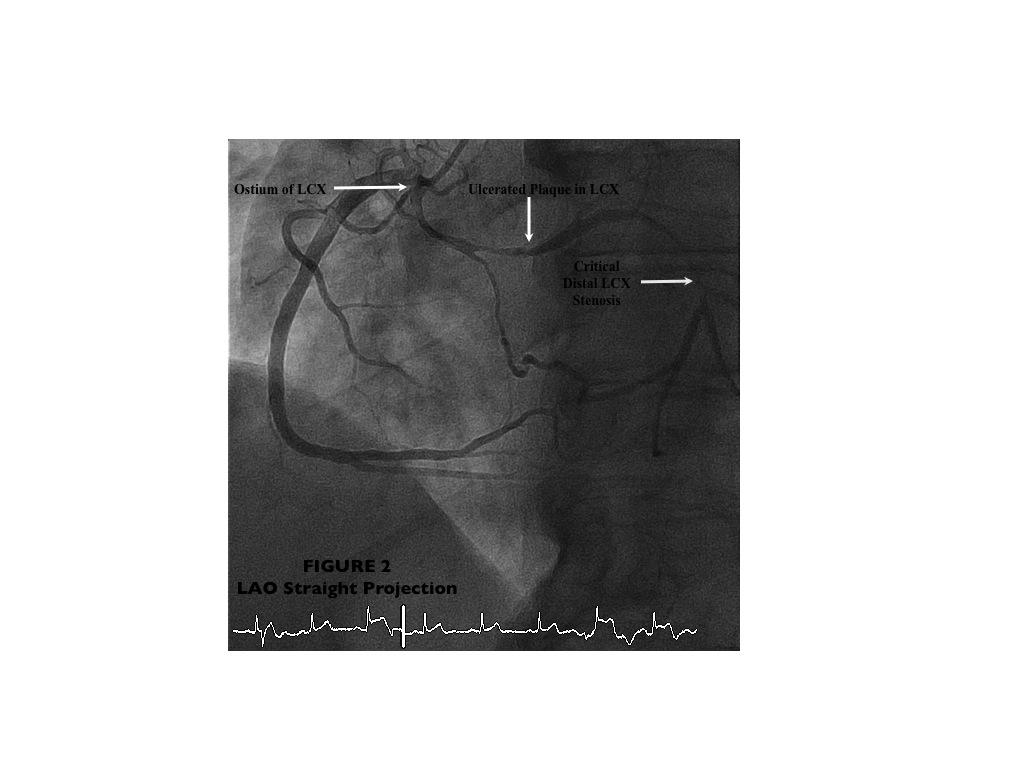
2. RCA was dominant with normal take off and no obstructive disease; however, the LCX arose from the proximal part of RCA (anomalous) and was severely and diffusely diseased with (1) 95-99% stenoses in mid and distal segments and (2) less severe, but also obstructive disease in its proximal part (Figure 2 is LAO straight projection).
2. RCA was dominant with normal take off and no obstructive disease; however, the LCX arose from the proximal part of RCA (anomalous) and was severely and diffusely diseased with (1) 95-99% stenoses in mid and distal segments and (2) less severe, but also obstructive disease in its proximal part (Figure 2 is LAO straight projection).
Procedure
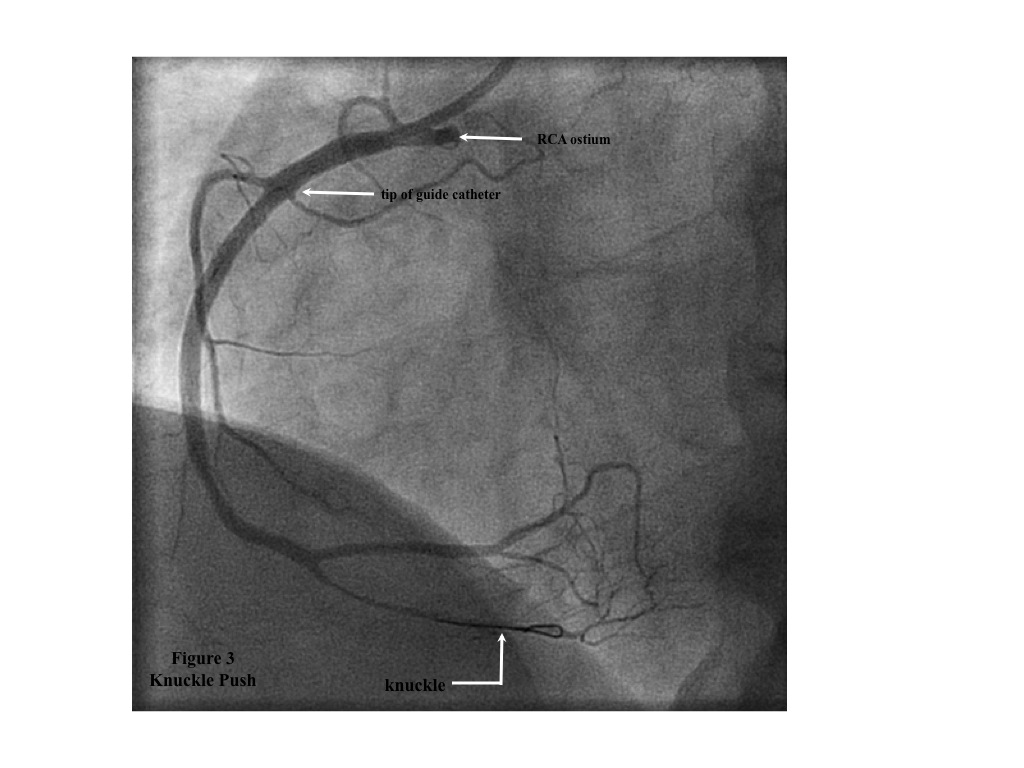
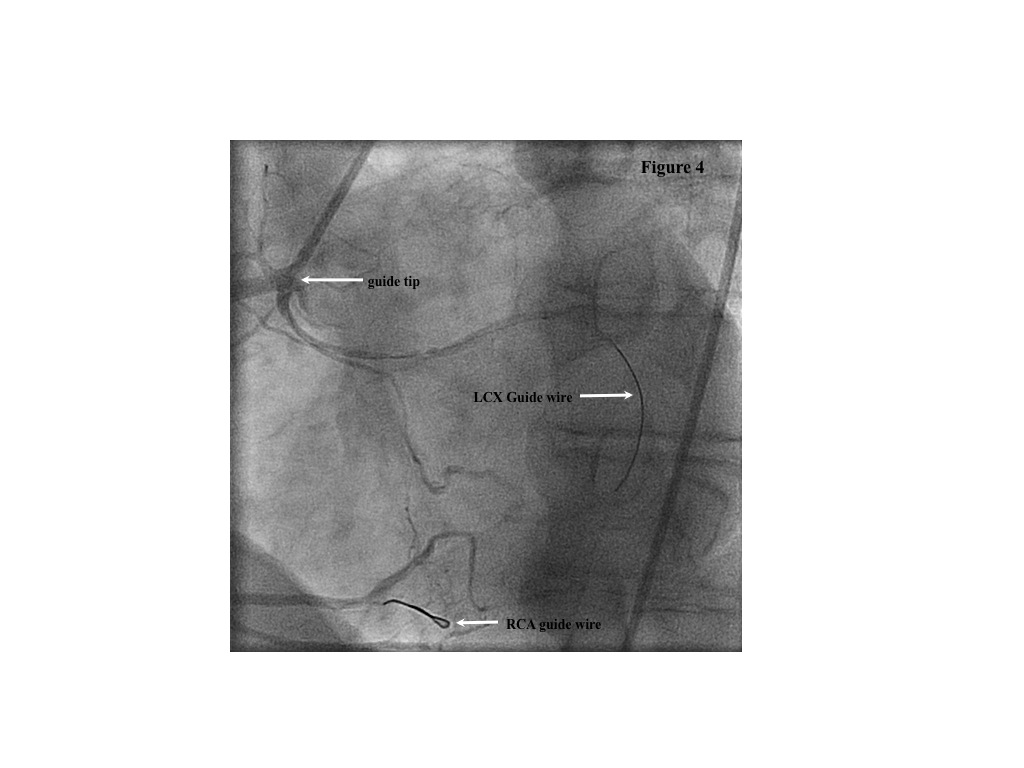
A 6Fr Multipurpose guiding catheter (MP 2) was inserted via right femoral artery access. This catheter had a tendency for deep intubation of the RCA (Figure 3). In order to avoid its prolapse into the unfavorable take off of the LCX (right angle between the proximal LCX and the guiding catheter, increasing the risk of LCX dissection), a BMW guidewire was placed into the distal RCA branc, with its distal end looped. By pushing this guidewire forward, the guiding catheter was controllably pushed out of the RCA to the level of the LCX take off. Once at this level, the LCX was wired with another BMW guidewire (Figure 4). The LCX was predilated with 2.0x15mm balloon and then stented with two Xience Primes 2.75x38mm (distal and mid) and a third Xience Prime 2.75x18mm (proximally) at high pressure.
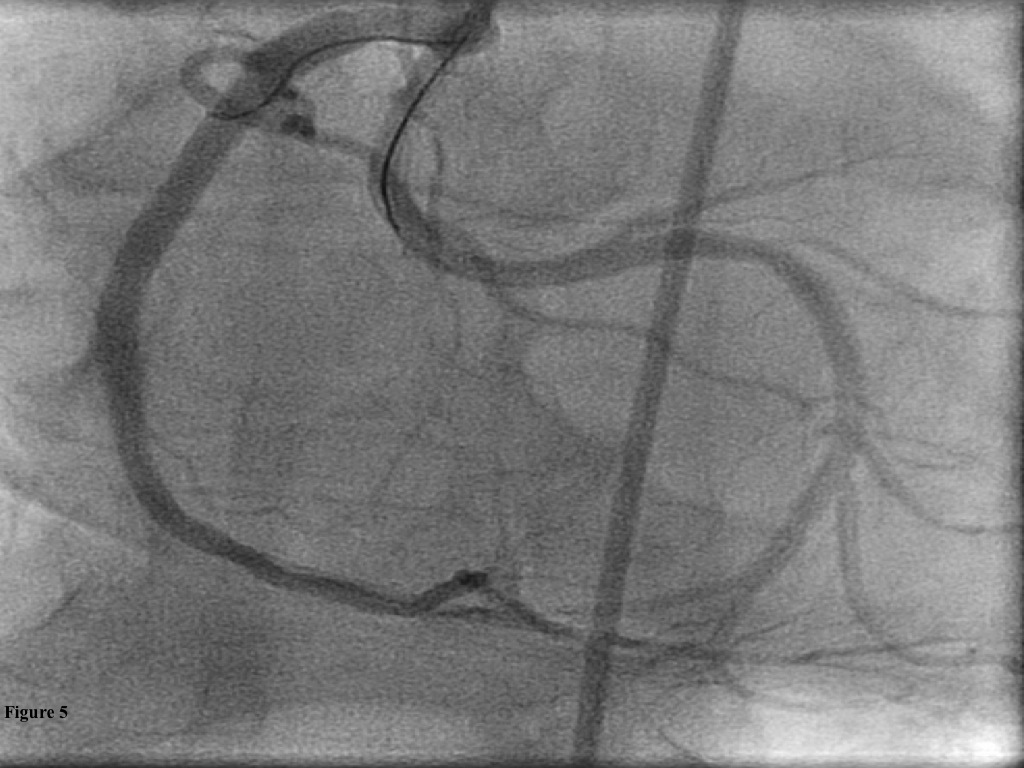
Conclusion(s) / Result(s)
The result was very satisfactory (Figure 5).
Comments/Lessons
An anomalous coronary artery take off may present a challenge for PCI, making the procedure more complex and risky. Choosing the guiding catheter is often a crucial step; however, since the catheter curves are designed for usual coronary anatomy, the guiding catheter might not fit well into an anomalous coronary ostium. Therefore, more advanced techniques may be needed to decrease the risk and increase the success of PCI. We present a case of acute coronary syndrome with LCX originating from proximal RCA as the culprit artery. By wiring the RCA first and using this guidewire to control the guiding catheter, safe and elegant positioning of the guiding catheter at the origin of the anomalous LCX was achieved. Then, once both vessels were wired, guiding catheter prolapse into LCX was prevented, and the stability of the system allowed for an uneventful completion of PCI.
Gallery
Conflicts of Interest
None
Comments