Bilateral Thrombotic Occlusion in STEMI: Staged Approach with Self-Expanding Stent
by
Gillian A. J. Jessurun
May 7, 2012Operator(s)
G. A. J. Jessurun, MD, PhD; A. Schramm, MD, PhD
Affiliation
Scheper ziekenhuis Emmen, The Netherlands
Facility / Institute
Scheper ziekenhuis Emmen, The Netherlands
Clinical History
A 62-year-old female patient with hypothyroidism, but no cardiac history was admitted. Risk factors included a positive family history and overweight. The patient had vague precordial complaints for about 1 week and assumed these were stomach complaints. The day before admission the patient visited her family physician because of chest pain. The electrocardiogram (ECG) was not interpreted as abnormal; however, during the first night of admission a second attack of chest pain was accompanied by an abnormal ECG. Physical examination revealed a BP of 110/65; heart sounds were normal, and no murmurs were detected. The patient was 85kg and 1.73cm tall. Laboratory examination results were as follows: creatine kinase (CK) 384 U/l; CK-MB 68 U/l; troponin T 281 ng/l. The patient was taking 0.125µg levothyroxine.
Angiography
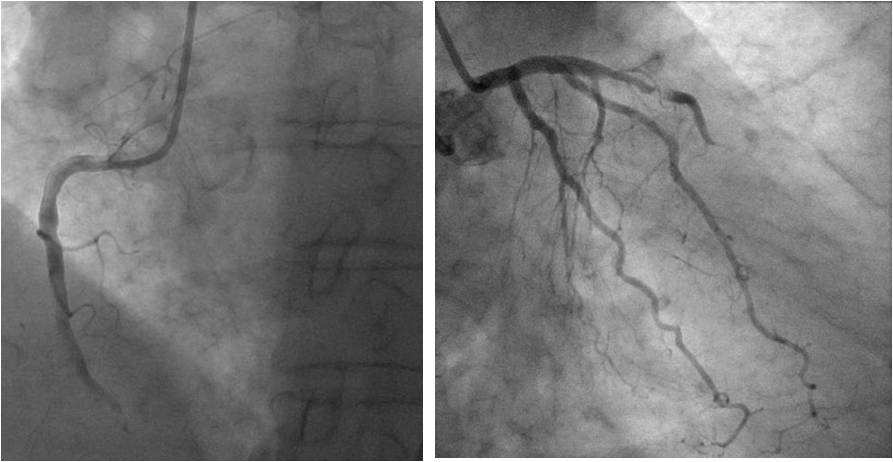
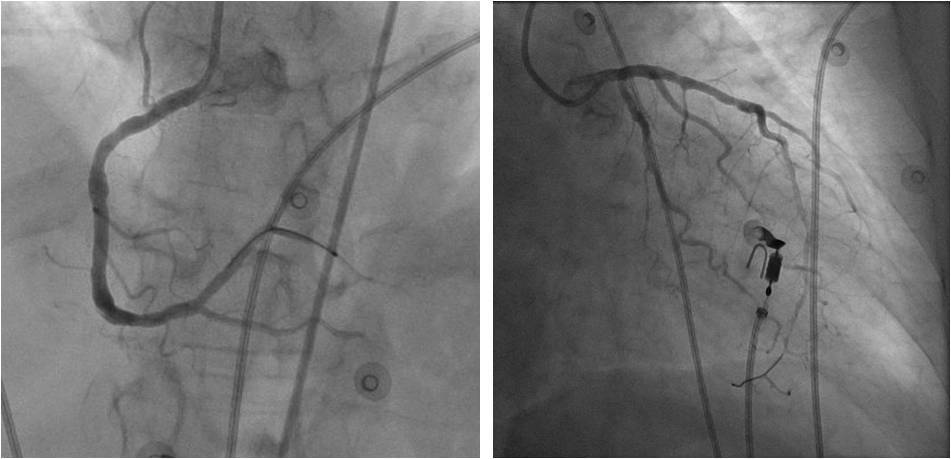
1) Subtotal thrombotic occlusion of the left anterior descending (Figure 1, right)
2) Total thrombotic occlusion of the RCA (Figure 1, left)
2) Total thrombotic occlusion of the RCA (Figure 1, left)
Procedure
The procedure was performed in two stages a few days apart:
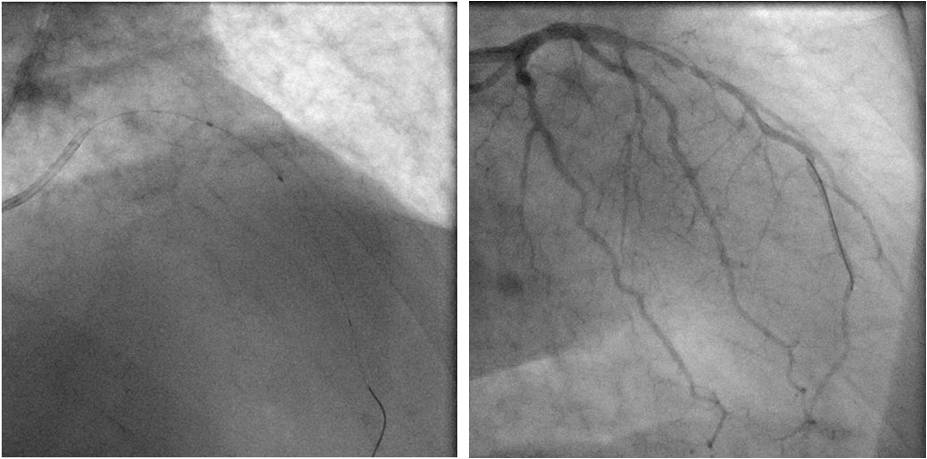
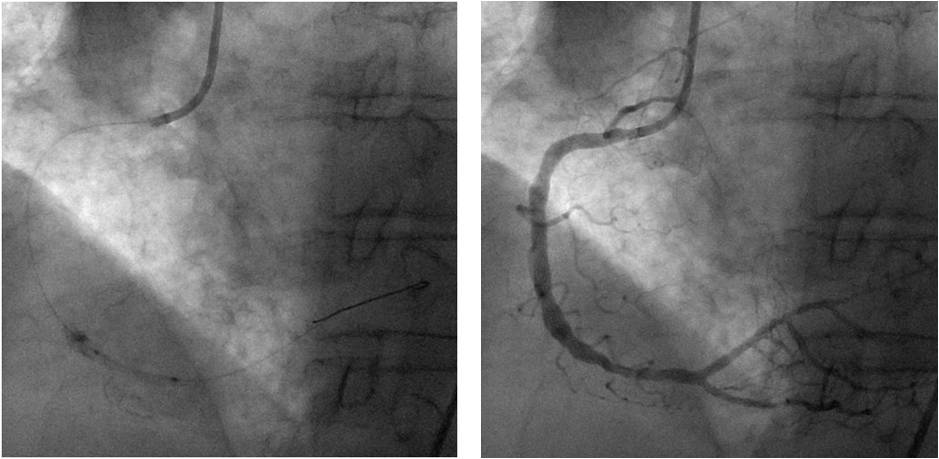
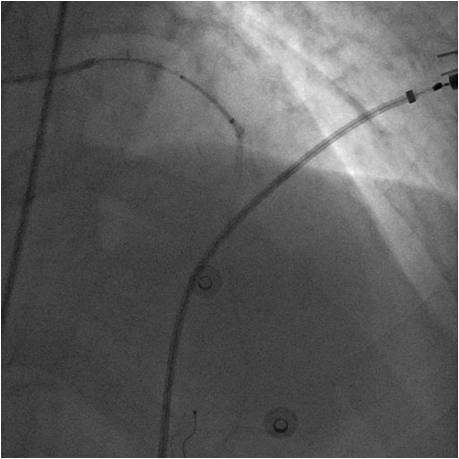
Stage 1: Aspiration using an Export AC (Medtronic) and predilation of the LAD (Figure 2) and the RCA (Figure 3) with IABP support.
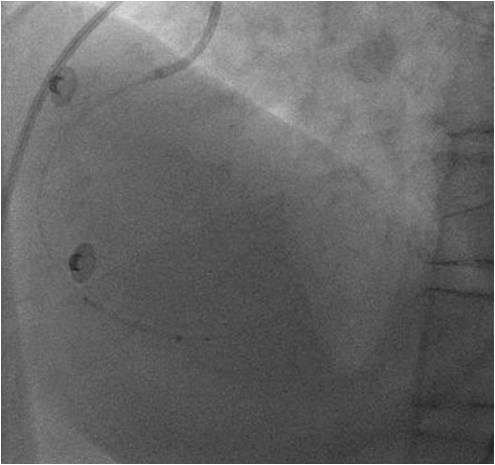
Stage 2: Implantation of self-expanding STENTYS stents in the RCA (Figure 4) and LAD (Figure 5).
The guiding catheters used were: GC JR4 and JL4 (Cordis). BMW guidewires (Abbott) were used for both stages. The stents used were STENTYS BMS 3.0–3.5 mmx27mm (RCA) and STENTYS 3.0–3.5mmx27mm (LAD).
The final result in the RCA and LAD (myocardial blush assessment) is shown in (Figure 6).
Stage 1: Aspiration using an Export AC (Medtronic) and predilation of the LAD (Figure 2) and the RCA (Figure 3) with IABP support.
Stage 2: Implantation of self-expanding STENTYS stents in the RCA (Figure 4) and LAD (Figure 5).
The guiding catheters used were: GC JR4 and JL4 (Cordis). BMW guidewires (Abbott) were used for both stages. The stents used were STENTYS BMS 3.0–3.5 mmx27mm (RCA) and STENTYS 3.0–3.5mmx27mm (LAD).
The final result in the RCA and LAD (myocardial blush assessment) is shown in (Figure 6).
Conclusion(s) / Result(s)
Echocardiography showed reasonable left ventricular function with normal dimensions and thrombus in the apex and an estimated ejection fraction of 50% and normal right ventricular function.
Comments/Lessons
1. STENTYS self-apposing stent reduces distal embolisation.
2. Angiographic underexpansion requires additional upsized low pressure ballooning.
3. Potential no reflow by additional ballooning may create conditions for a staged procedure.
2. Angiographic underexpansion requires additional upsized low pressure ballooning.
3. Potential no reflow by additional ballooning may create conditions for a staged procedure.
Gallery
Conflicts of Interest
This clinical case study has been submitted with support from STENTYS.
Comments