Distal Embolic Protection in SVG Intervention
by
Nafe Ashour
April 8, 2013Operator(s)
Nafe Ashour, MD; Daniel Möller ,MD
Affiliation
Katharinen-Hospital Cardiology Department, Unna ,Germany
Facility / Institute
Katharinen-Hospital Cardiology Department, Unna ,Germany
Clinical History
A 73 year old diabetic and normotensive man presented with a history of chest pain with duration of 2 weeks. Dobutamine stress testing induced anterior wall motion abnormalities. He had undergone CABG four years previously with SVG to LAD, SVG to LCX, and SVG to RCA.
Angiography
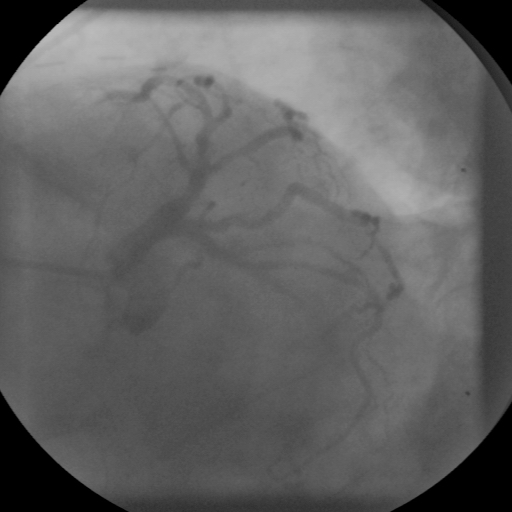
1) LAD: total occlusion after the large first diagonal (Figure 1)
2) LCX: occluded after OM1.
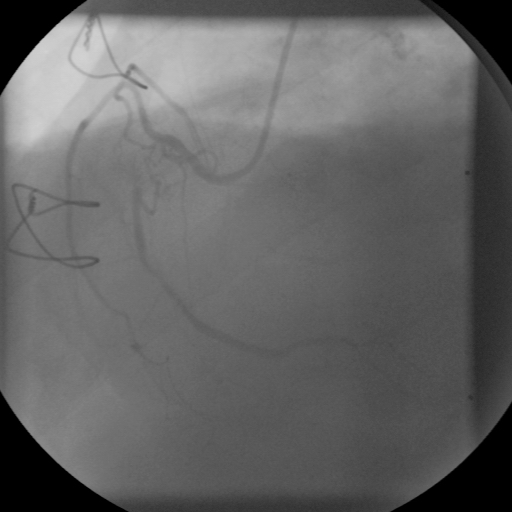
3) RCA: mid-chronic total occlusion (Figure 2)
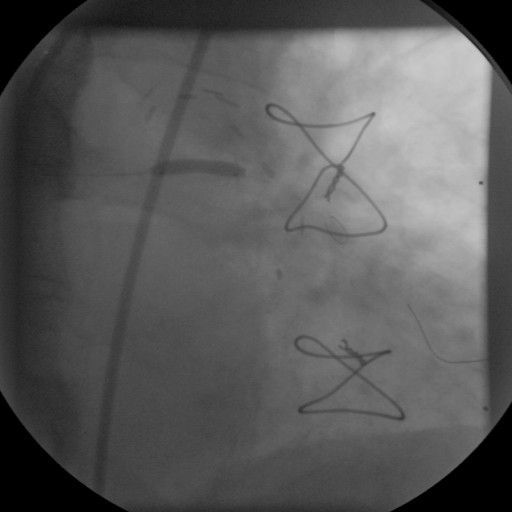
4) SVG to LAD: proximal 90% stenosis (Figure 3)
5) SVG to LCX: patent
4) SVG to RCA: occluded
2) LCX: occluded after OM1.
3) RCA: mid-chronic total occlusion (Figure 2)
4) SVG to LAD: proximal 90% stenosis (Figure 3)
5) SVG to LCX: patent
4) SVG to RCA: occluded
Procedure
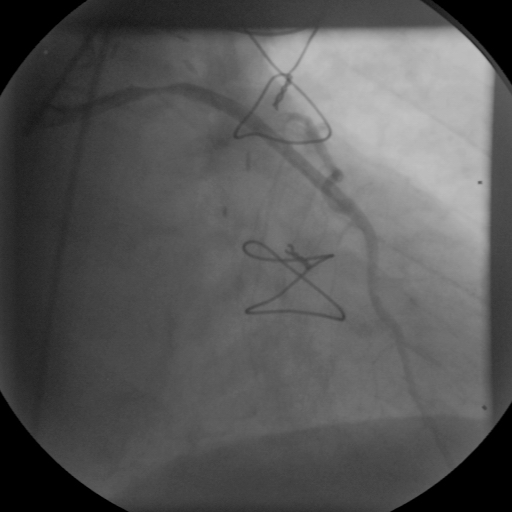
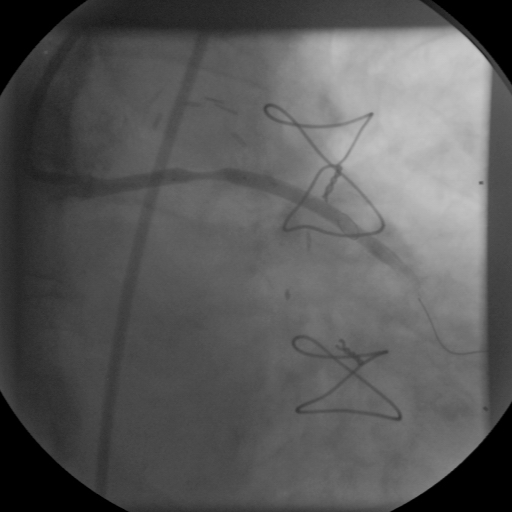
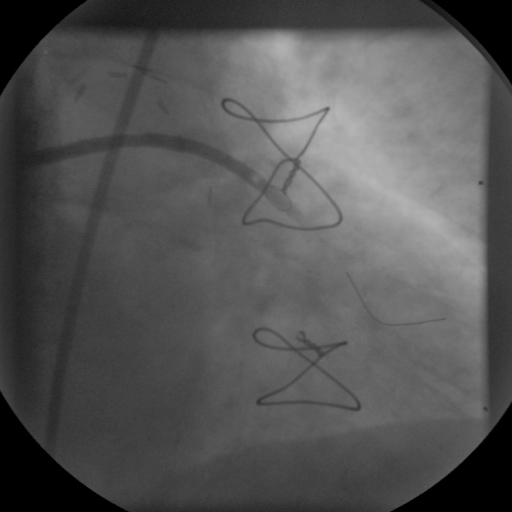
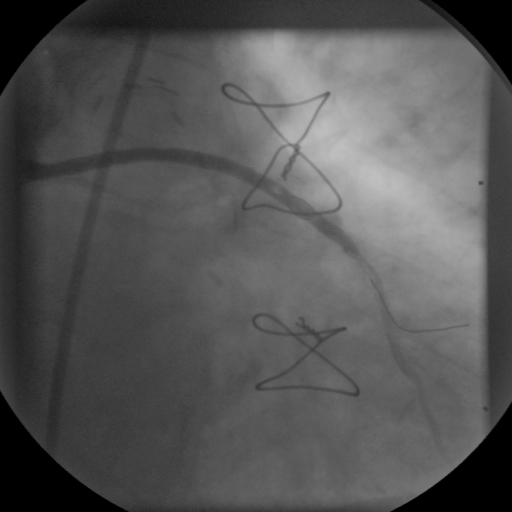
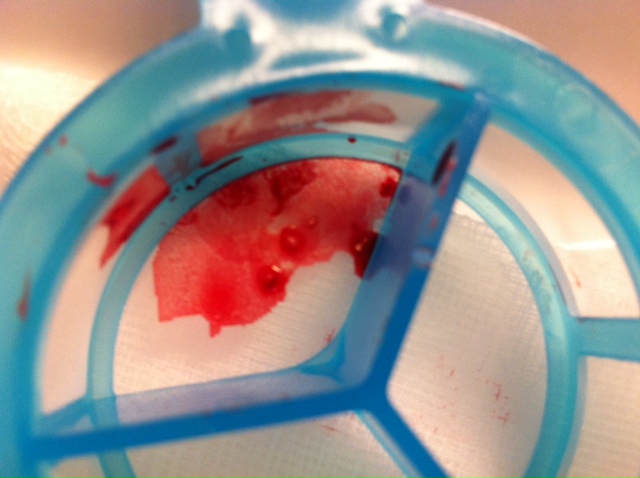
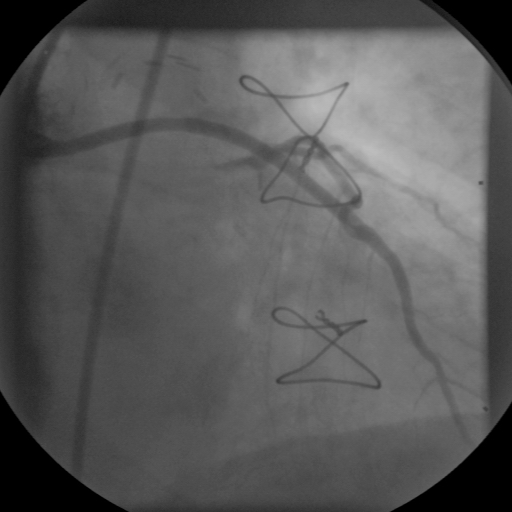
The SVG to LAD was cannulated using a 6Fr JR4 SH guiding catheter. After a distal protection device (Filter wire EZ 3.5-5.5 mm, Boston Scientific) was positioned (Figure 4), the mid SVG lesion was directly stented with a 3.0x15mm Pro-Kinetic (BMS) to 18 atm (Figure 5). After stent placement the angiogram showed slow flow and thrombotic material proximal to the filter wire (Figure 6, Figure 7) . We suspected this phenomenon was induced by partial obliteration of filter pores by atherosclerotic emboli. After retrieval of the FilterWire EZ, whitish debris was noted within the basket (Figure 8). and distal TIMI III flow was achieved (Figure 9).
Conclusion(s) / Result(s)
The patient tolerated the procedure well with no complications.
Comments/Lessons
SVGs are not like native arteries, SVGs can often stenose within 3 years and 50% may occlude by 10 years. Morphologically, SVG lesion tends to be diffuse, concentric, and friable with poorly developed or absent fibrous cap. SVG lesions have a high embolic risk. Distal embolization can cause microvascular obstruction via plugging with secondary spasm and platelet aggregation and clinical complications such as no-reflow and peri-procedural MI. The embolic event cannot be accurately predicted by clinical or angiographic variables. Mechanical embolic protection devices are used to try to capture the atheroemboli that are liberated during the SVG intervention.
Gallery
Conflicts of Interest
None
Comments