Distal LMCA Bifurcation Stenosis Treated with a Crush Technique
by
Nelson Carrillo Manzano
June 24, 2013Operator(s)
Nelson Carrillo Manzano, MD; Roberto Richiusa, MD
Affiliation
Centro Médico Loira, Caracas, Venezuela
Facility / Institute
Centro Médico Loira, Caracas, Venezuela
Clinical History
A 81 year old male patient with a history of hypertension, dyslipidemia, and smoking, presented with a history of chest pain with minimal efforts of two days duration. ECG showed negative T waves I-AVL and V5-V6.
Angiography
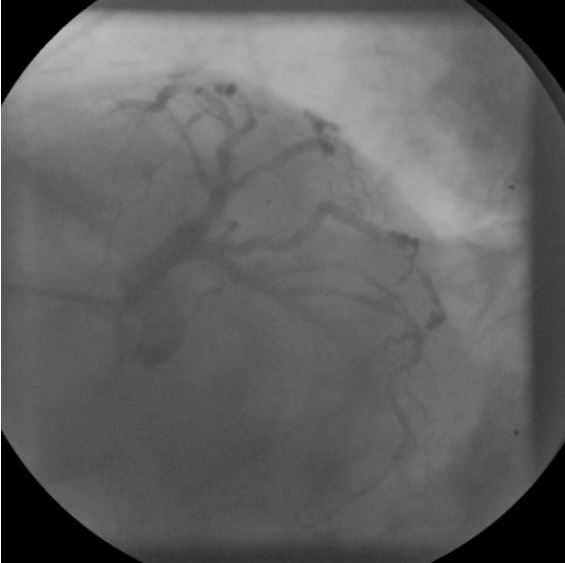
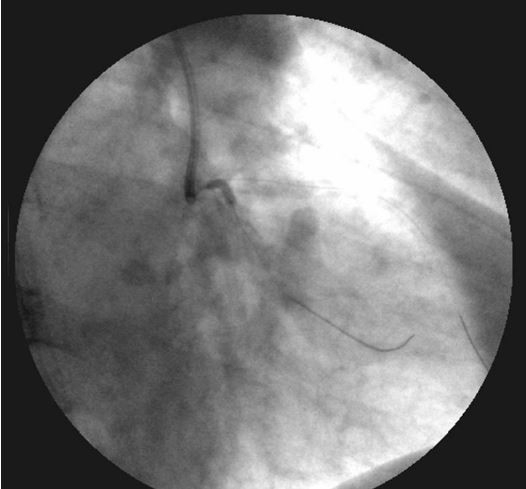
1- LM: distal 95% stenosis, involving the origin of LAD and LCX: bifurcated lesion type 1-1-1. (figure 1)
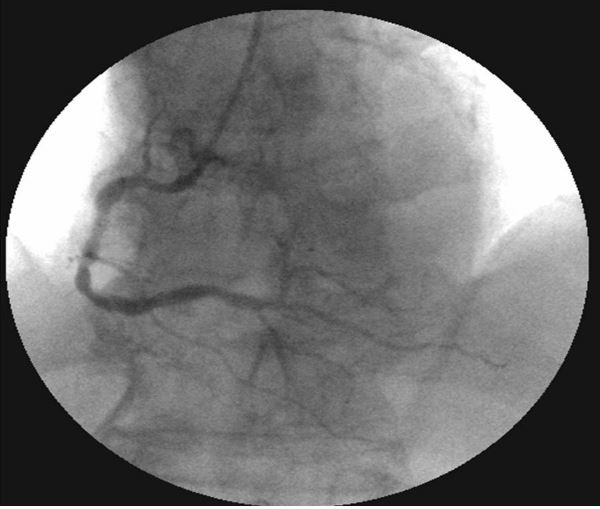
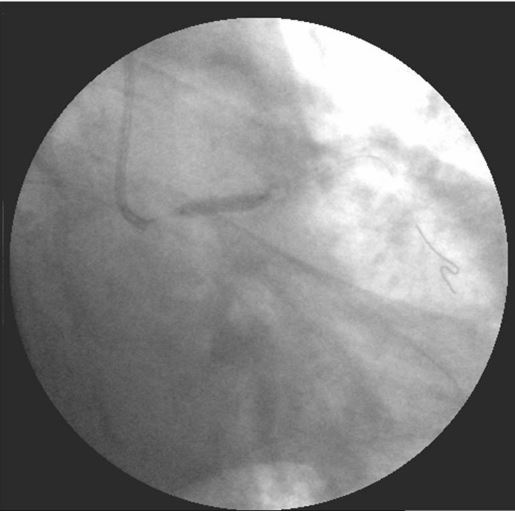
2- LAD: ostial 90% stenosis and mid 60%. Severely calcification. (figure 2)
3- LCX: ostial 90% stenosis and mid 80% stenosis.
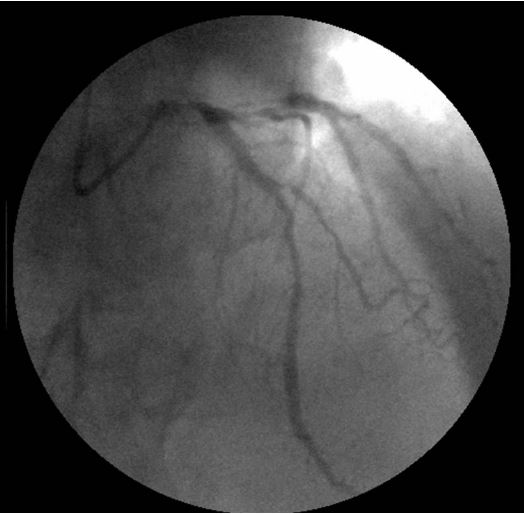
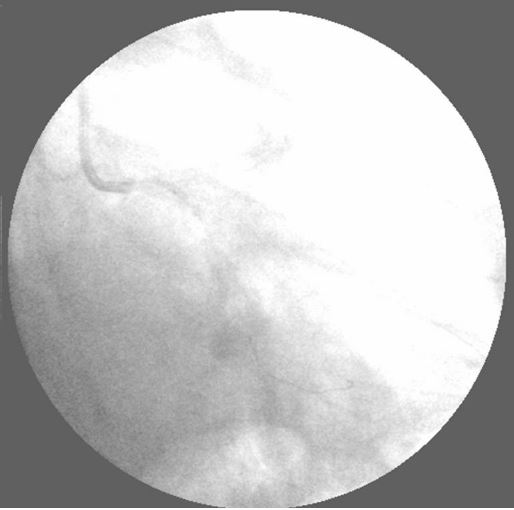
4- RCA: mid 30% tandem stenoses. (figure 3)
2- LAD: ostial 90% stenosis and mid 60%. Severely calcification. (figure 2)
3- LCX: ostial 90% stenosis and mid 80% stenosis.
4- RCA: mid 30% tandem stenoses. (figure 3)
Procedure
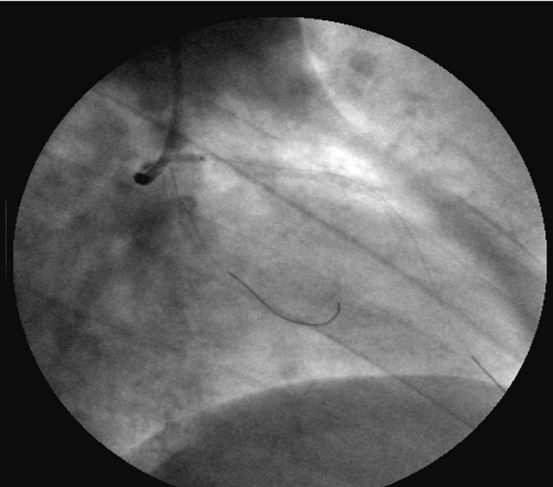
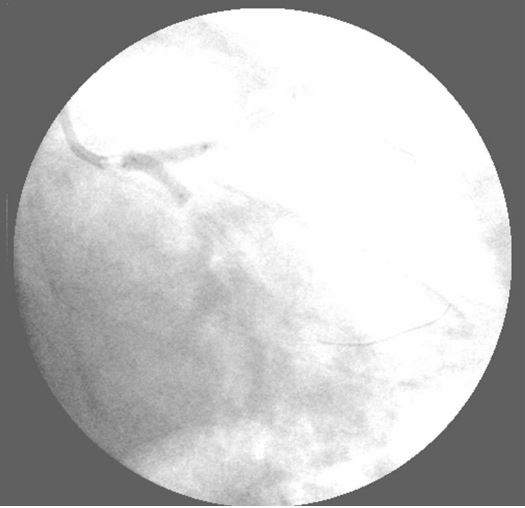
A 7Fr, Medtronic Launcher EBU 3.5 guiding catheter was used to engage the LM. A BMW Universal guidewire was postioned into the distal LAD. Another BMW Universal guidewire was positioned into the distal LCX. A 2.5x15mm Sprinter Legend balloon was used to dilate the ostial LAD (figure 4) and ostial LCX (figure 5) lesions. Next a 3.0x20mm Apex balloon was used to dilate the mid LCX lesion (figure 6). Then a 3.5x23mm Xience Prime stent was passed into the mid LCX and deployed at 16atm (figure 7, figure 8). Two stents were then positioned simultaneously (figure 9): first a Xience Prime 3.5x16mm was positioned from the mid LM to the ostium of the LCX and deployed at 16atm (figure 10). LCX guidewire was removed and the second stent was positioned: a 3.5x16mm Promus Element from the Mid LM to LAD ostium and deployed at 16atm, crushing the proximal end of the first stent (figure 11). A Whisper guidewire was passed through the struts into the LCX; and the ostial LCX was predilated with a 1.5x15mm Sprinter Legend balloon (figure 12). Finally kissing balloon inflations were performed using a 3.5x15mm Apex balloon from the mid LM to the ostial LAD and a second 4.0x15mm Sprinter balloon from mid LM to ostial LCX (figure 13).
Conclusion(s) / Result(s)
Good angiographic result with a TIMI 3 flow.
Comments/Lessons
The crush technique is our first choice in the treatment of complex bifurcation lesion of left main.
Gallery






Conflicts of Interest
No conflict of interest
Comments