Double Bifurcation Treated with Two Tryton Side-Branch Stents
by
García Fernández
January 7, 2013Operator(s)
E. García Fernández, L. Unzué Vallejo
Affiliation
Hospital Universitario Madrid Montepríncipe, Madrid, Spain
Facility / Institute
Hospital Universitario Madrid Montepríncipe, Madrid, Spain
Clinical History
A 48-year-old-man with hypertension was admitted to our center with a positive stress test. Six months before he presented with sudden cardiac arrest at which time coronary angiography was described to show moderate disease in the proximal and distal left anterior descending artery (LAD) and chronic total occlusion of the right coronary artery (RCA) treated successfully with 1 drug eluting stent; transthoracic echocardiography showed inferior akinesia with normal systolic left ventricular function (LVEF=80%); and an ICD was implanted before discharge. The patient remained asymptomatic since then; a stress test was clinically negative, but electrically positive.
Angiography
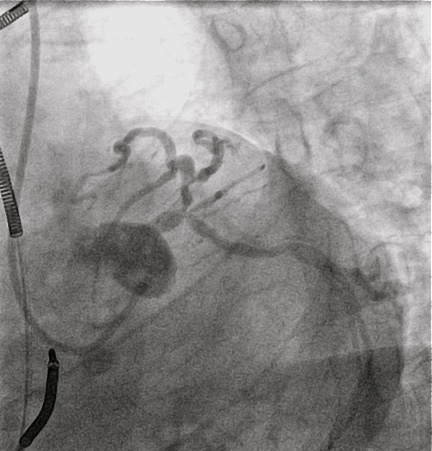
LMCA: Short, calcified, with severe stenosis of the distal segment involving the bifurcation and the ostia of the left circumflex (LCX), left anterior descending (LAD), and a small ramus (Medina 1,1,1) (Figure 1).
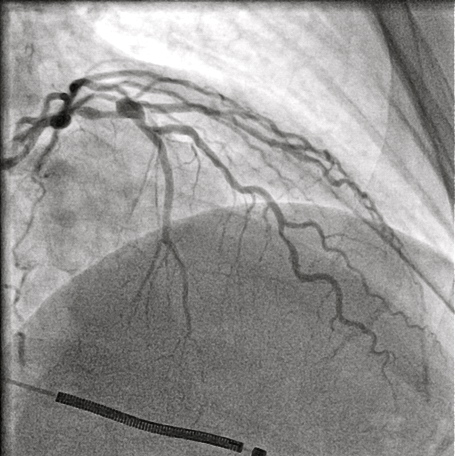
LAD: large vessel with moderate stentosis involving the bifurcation of a large diagonal (D1) that had a critical ostial stenosis (Medina 1,1,1) followed by aneurysmal dilatation of the middle LAD with severe stenosis in the distal LAD (Figure 2).
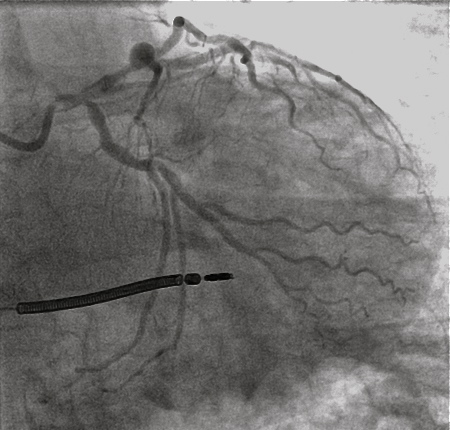
LCX: large vessel, with severe ostial stenosis (Figure 3).
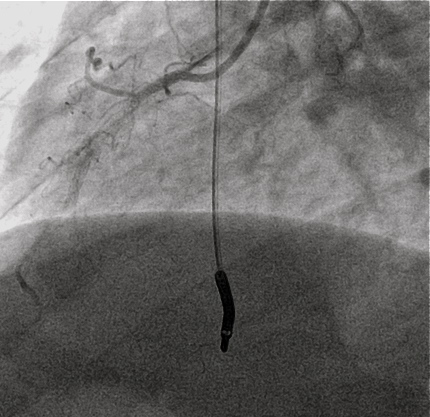
RCA: dominant vessel, with occlusive in-stent restenosis (ISR) retrograde filling of the posterior interventricular and posterolateral branches from collaterals (Figure 4).
LAD: large vessel with moderate stentosis involving the bifurcation of a large diagonal (D1) that had a critical ostial stenosis (Medina 1,1,1) followed by aneurysmal dilatation of the middle LAD with severe stenosis in the distal LAD (Figure 2).
LCX: large vessel, with severe ostial stenosis (Figure 3).
RCA: dominant vessel, with occlusive in-stent restenosis (ISR) retrograde filling of the posterior interventricular and posterolateral branches from collaterals (Figure 4).
Procedure
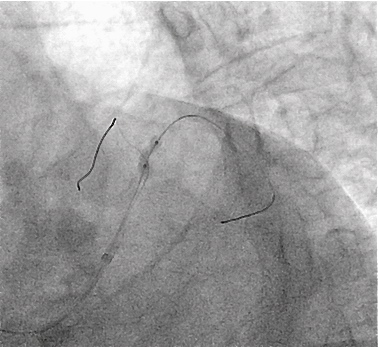
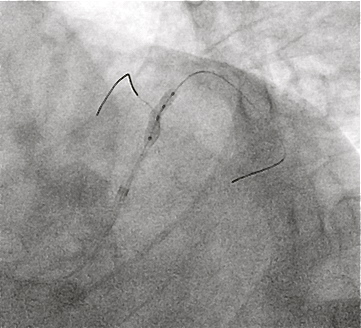
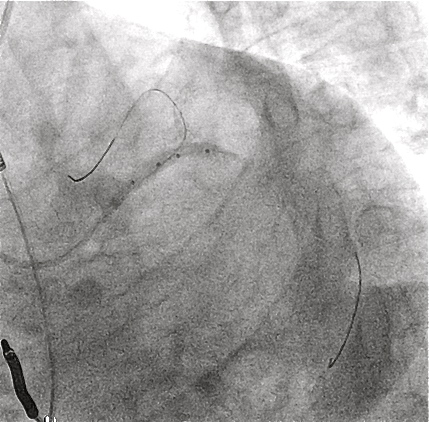
The LMCA was engaged with an EBU 3.5 6 Fr guiding catheter through right radial approach. A PT 2 guidewire was placed in the first diagonal branch, and a BMW guidewire was placed in distal LAD. Predilation of both vessels was performed with a 2.5x12 Sprinter balloon at 12atm (Figure 5). A Tryton Side Branch stent 2.5-3.0 was deployed at 12 atm in the first diagonal with a good angiographic result (Figure 6). The PT 2 guidewire was then placed in the LCX with predilation of the LCX ostium with the Sprinter balloon at 12 atm. A second Tryton Branch stent 3.0-3.5 was implanted in the LCX with good flexibility and trackability of the stent through the calcified lesion (Figure 7). After that, wires were recrossed, and the LMCA was predilated with a non-compliant balloon (Hiryu 3x15 at 16 atm). Finally, a Resolute Integrity 3x30mm stent was implanted at the LM-LAD covering both bifurcations with the proximal struts covering the aorto-ostial transition. The procedure concluded with kissing balloon post-dilation of both bifurcations (LM-LCX Hiryu at 24atm and Sprinter at 18atm; LAD-Diagonal Hiryu at 16atm and Sprinter at 14atm) with a good angiographic result (Figure 8).
Procedure time: 55 min. Fluoroscopy time: 16 min. Contrast dose: 120 cc Hexabrix.
Procedure time: 55 min. Fluoroscopy time: 16 min. Contrast dose: 120 cc Hexabrix.
Conclusion(s) / Result(s)
The patient was discharged the day after the procedure taking 10mg/d prasugrel and 100mg/d aspirin.
Comments/Lessons
Treatment of bifurcation lesions with the Tryton side branch stent has been shown to be feasible with an acceptable clinical outcome and low side branch late loss. The use of the Tryton side branch stent for treatment of LM bifurcation disease in combination with a conventional drug eluting stent is feasible and results in an optimal angiographic appearance.
The Tryton-LM multicenter registry is ongoing, with good angiographic results and acceptable outcome at short-term follow-up. To our knowledge, this is the first case where two bifurcations are treated with two Tryton Sidebranch stents in the same patient at the same time, covering the main vessel with a conventional drug-eluting stent.
The Tryton-LM multicenter registry is ongoing, with good angiographic results and acceptable outcome at short-term follow-up. To our knowledge, this is the first case where two bifurcations are treated with two Tryton Sidebranch stents in the same patient at the same time, covering the main vessel with a conventional drug-eluting stent.
Gallery

Conflicts of Interest
None
Comments