LIMA Stenting Through a Left Radial Approach After PCI of an LAD Through a LIMA Caused a Severe Dissection
by
Saidur Khan
November 5, 2012Operator(s)
Dr. Saidur Rahman Khan
Affiliation
Ibrahim cardiac Hospital and Research Institute, Dhaka, Bangladesh
Facility / Institute
Ibrahim cardiac Hospital and Research Institute, Dhaka, Bangladesh
Clinical History
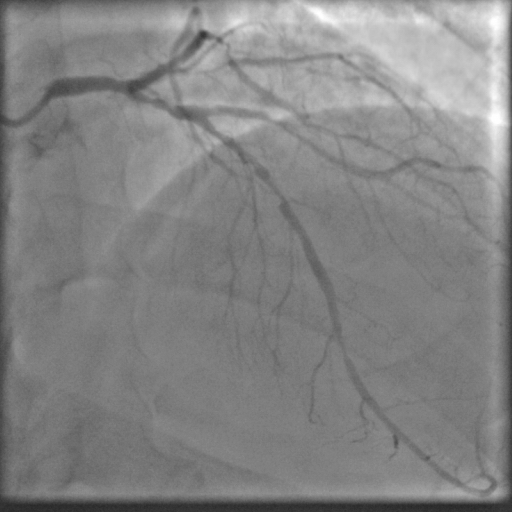
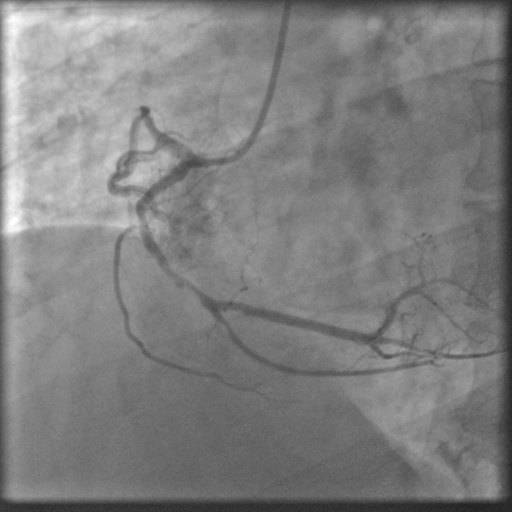
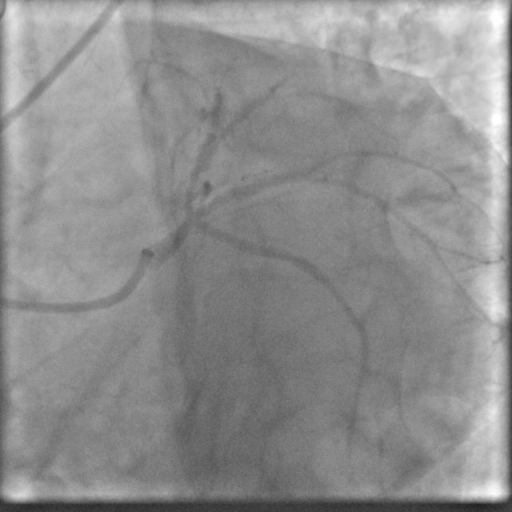
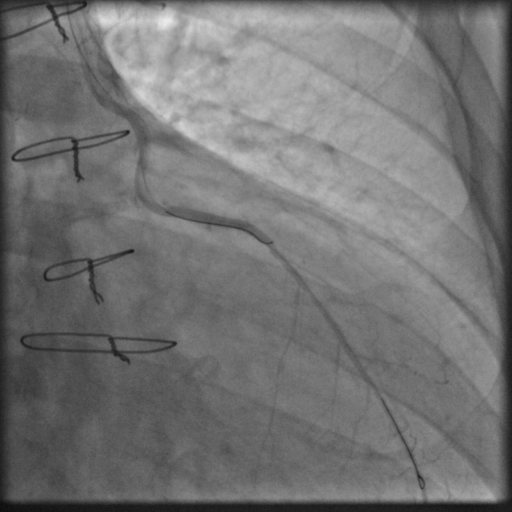
A 52 year old male, hypertensive, diabetic gentleman was admitted into our hospital with complaints of typical angina. He was hemodynamically stable with dynamic ST-T changes in anterolateral leads with no elevation of Troponin I and an LVEF of 60%. He previously underwent CABG with 4 grafts - LIMA to LAD, SVG to OM, D1 and RCA - after angiography revealed a severely diseased proximal-mid LAD and a 80% stenosis in the distal LAD and severely diseased ramus and RCA (Figure 1, Figure 2).
Angiography
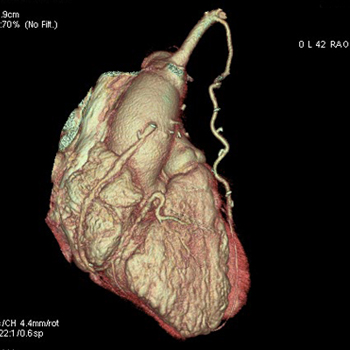
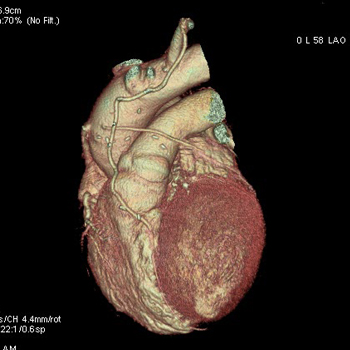
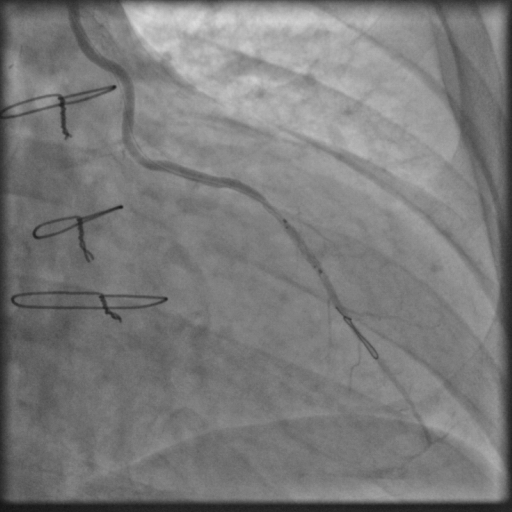
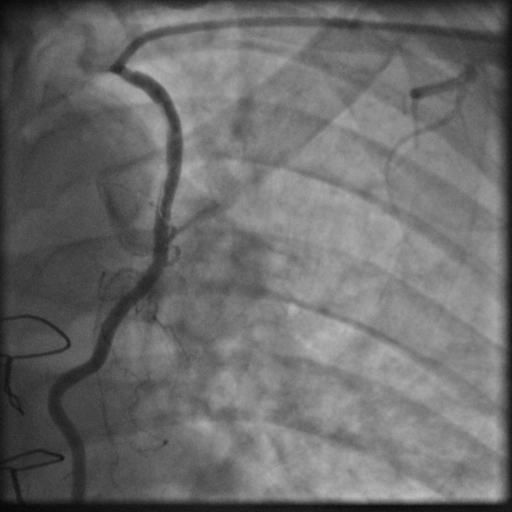
CT angiography revealed a patent LIMA to the LAD with an 80% stenosis in the distal LAD (he LIMA graft was implanted in mid LAD with no skip graft for the distal LAD lesion), an occluded SVG to the diagonal, a diffusely diseased SVG to OM with feeble distal runoff in the OM, and a mildly diseased SVG to RCA proximally (Figure 3, Figure 4). The ramus was severely diseased.
Procedure
Using the left radial approach a 6Fr JL 3.5 guiding catheter, and a BMW guidewire, the lesion in the ramus was crossed and predilated using a 1.5x10mm Sapphire balloon. The target lesion was stented using a 2.25x18mm Euca Tax stent (PES, Germnay) at 14atm to achieve TIMI III flow (Figure 5, Figure 6). Then a 5Fr JR guiding catheter was used to cannulate the LIMA. A BMW guidewire was chosen to cross the LAD lesion through the LIMA. Due to the tortuosity of the LIMA, this required support with a 2x9mm Maverick balloon after which the target lesion was predilated at 12atm. Then an attempt was made to deploy a 2.5x12mm Optima stent (CID, Italy), but it was very difficult even using “buddy wiring” technique. Deep intubation of the guiding catheter was required to position the stent that was then implanted at 16atm (Figure 7, Figure 8). After the guiding catheter and guidewire were withdrawn, there was no flow to the LIMA (Figure 9). After rewiring, a long segment of intimal dissection in the LIMA was observed (Figure 10). Therefore, two bare metal stents (3x23mm STS Flex and 3x18mm R stent) were deployed into the LIMA overlapping each other (Figure 11, Figure 12). Distal TIMI III flow was achieved.
Conclusion(s) / Result(s)
During this eventful procedure of one and a half hour, patient cooperated properly without any hemodynamic instability. No ischemic changes in the ECG were observed after PCI. The patient was discharged 2 days after PCI. Follow up after 2 weeks was done, and the patient was symptom free.
Comments/Lessons
Left radial approach specially for graft study in post CABG patients is a popular alternative to femoral access. This is the first time that this operator experienced a dissection of the LIMA during PCI. Possibly the angulation of the LIMA along with deep intubation of the catheter caused this disaster. There are no trials to indicate whether DES is necessary for LIMA stenting. Cautious use of the guiding catheter is very important for preventing this sort of event.
Gallery




Conflicts of Interest
None
Comments