A Mess of a Clot
by
Omar Hasan
May 29, 2012Operator(s)
Omar Hasan, Aadil Shaukat
Affiliation
Victoria Infirmary, Glasgow, UK
Facility / Institute
Cardiology Department, Victoria Infirmary, Glasgow, UK
Clinical History
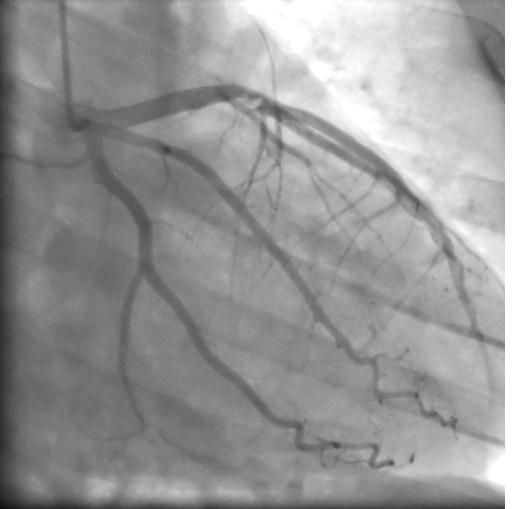
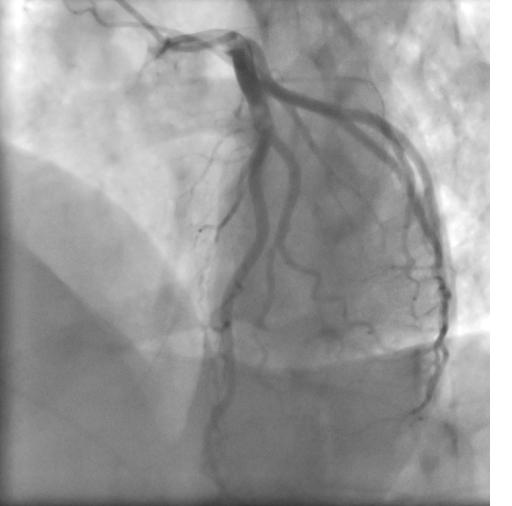
A 33 year old ex-smoking male of Asian background was admitted with resting chest pain. His ECG did not show acute ischemia, but the troponin I level was mildly raised to 0.61. He underwent primary angioplasty to the LAD two years ago. His angiogram at that time showed a thrombotic occlusion of his mid LAD (Figure 1, Figure 2) that was treated that with manual aspiration, balloon dilation, and stenting across a moderate sized diagonal. He did well following the procedure, and suffered a limited anteroseptal infarct with relatively preserved left ventricluar systolic function. His echocardiogram otherwise was reported as normal.
Angiography
Right radial artery access
LMCA, LCX, and RCA were all smooth and normal.
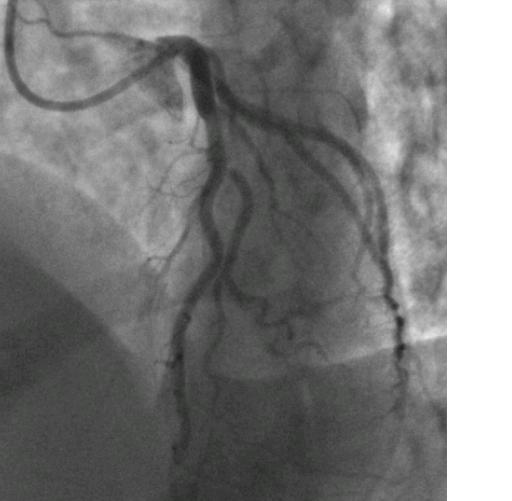
LAD: The stent was widely patent in the mid-course; however, the jailed diagonal origin was pinched but with TIMI 3 flow (Figure 3).
LMCA, LCX, and RCA were all smooth and normal.
LAD: The stent was widely patent in the mid-course; however, the jailed diagonal origin was pinched but with TIMI 3 flow (Figure 3).
Procedure
Repeat echocardiography was performed which showed an obvious atrial septal defect in the secundum region with left to right flow. The right ventricle was dilated with some pressure overload features.
Conclusion(s) / Result(s)
Patient is listed currently for an ASD closure procedure
Comments/Lessons
Critical review of his initial angiogram showed the LAD occlusion to be thrombotic in origin with no plaque or disruption at the site of occlusion. The most likely initial presentation 2 years ago was a paradoxical embolus through ASD into the LAD. The echocardiogram at that time overlooked the ASD altogether. Paradoxical emboli into the coronary arteries is an exceedingly rare phenomenon. Yet the index of suspicion should be high in acute cases with pure thrombotic occlusion of coronaries. The echocardiogram should be carried out to high standards and further diagnostics like bubble contrast study should be done to explore possibility of a clinically significant PFO even.
Gallery
Conflicts of Interest
None
Comments