PCI of High Take-Off RCA from Left Coronary Sinus with Acute Inferior Wall MI
by
Sridhar Kasturi
September 7, 2015Operator(s)
Sridhar Kasturi, MD, DM, FACC
Affiliation
SHK Hospitals, Hyderabad.
Facility / Institute
Sun Shine Heart Institute, Paradise,Secunderabad, Andhra Pradesh, India
Clinical History
37 yr old normotensive, euglycemic female patient was referred for acute inferior wall MI with recurrent angina status post treatment with streptokinase. Her physical examination at the time of admission showed stable vital signs with HR-70/min, BP -130/80mmHg, heart sounds normal, lungs-clear. Investigations revealed ECG-NSR, Q waves with ST elevations in inferior leads; chest x-ray- within normal limits; creatinine-0.9mg/dl, troponin T positive, CPK-MB-48mg/dl; 2D echocardiogram- regional wall motion abnormalities of inferior & posterior wall with good LV function, EF – 60%; carotid doppler – normal.
Angiography
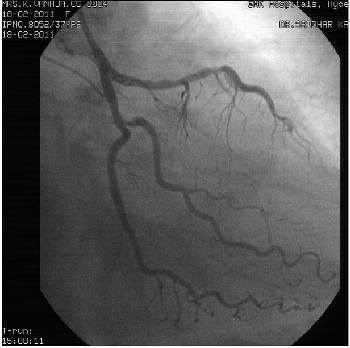
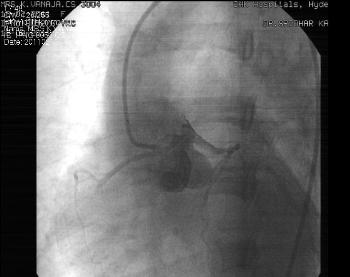
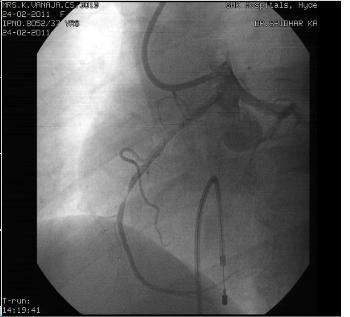
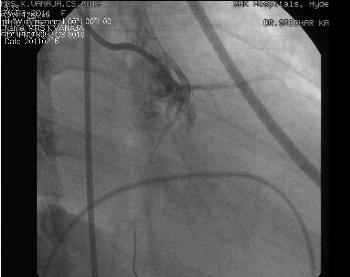
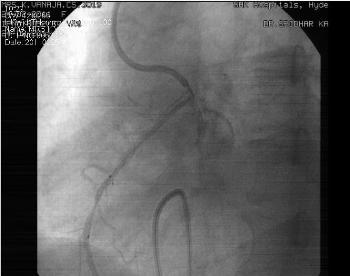
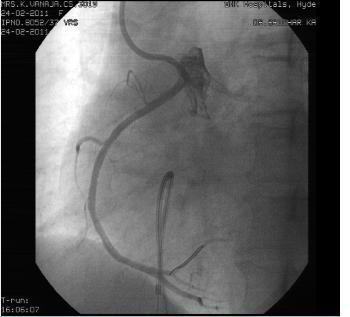
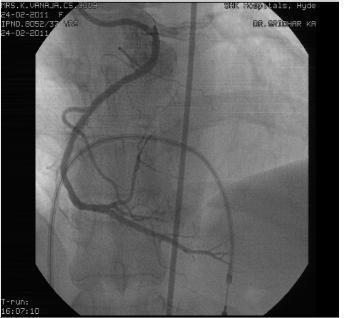
Angiogram was done through right femoral approach revealed LMCA – Normal, LAD – Type-III, mild proximal disease, LCX – non dominant, ostial 60% narrowing of OM branch, RCA – anomalous dominant, arising high above left coronary sinus with mid total occlusion, retrograde filling of distal RCA through LCA collaterals (Figure 1, Figure 2, Figure 3, Figure 4).
Procedure
PTCA with stenting of mid RCA was done through right femoral approach with temporary pacemaker support. We faced great difficulty in engaging RCA due to anomalous high origin above left coronary sinus (Figure 5) resulting in kinking, coiling and distorted shaping of various guide catheters. We used 6Fr AR, AR2, AL2, JL3, XB3.5, JR, multipurpose Hockeystick II and RBV guide catheter but failed in getting adequate alignment (Figure 6,Figure 7). Finally, we succeeded using an AL1, 6Fr guide catheter. Mid RCA lesion was stented with AXXION (paclitaxel coated) 2.75mm x 18mm at 10 to 14atms pressure inflations (Figure 8). Post stent angiogram showed TIMI grade III flow without any complications (Figure 9, Figure 10).
Conclusion(s) / Result(s)
Post procedure stay was uneventful. Patient was discharged on 5th day of procedure with aspirin, clopidogrel and ACE inhibitors & statin therapy.
Comments/Lessons
Anomalous origin of RCA from left sinus, or high origin, is associated with sudden death and myocardial infarction due to course of RCA through great arteries. Sometimes kinking and slit like opening of proximal RCA also contributes to sudden death and myocardial ischemia. During CAG and PCI the best way to engage anomalous RCA is with left amplatz catheter instead of using other catheters which will be time saving with less complications.
Gallery



Conflicts of Interest
N/A
Comments