PCI to SVG by Left Radial Approach Using Distal Protection Device
by
Saidur Rahman Khan
May 14, 2012Operator(s)
Saidur Rahman Khan, MD
Affiliation
Ibrahim cardiac Hospital and Research Institute, Dhaka, Bangladesh
Facility / Institute
Ibrahim cardiac Hospital and Research Institute, Dhaka, Bangladesh
Clinical History
A 44 year woman was admitted with complaints of chest pain. Her cardiac markers were raised, and ECG showed dynamic ST-T changes in the inferolateral leads. She had undergone CABG 4 years previously with LIMA to LAD and SVG to LCX (OM).
Angiography
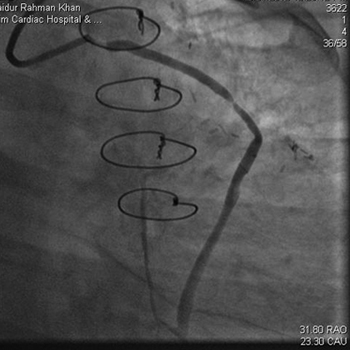
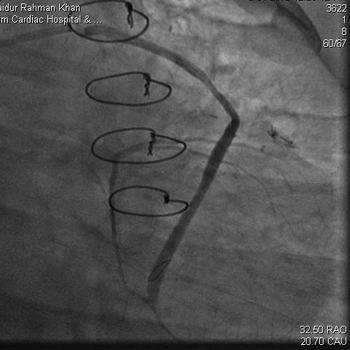
1) Occluded LAD and LCx from their ostia
2) Patent LIMA to LAD with good antegrade flow into the distal LAD.
3) No significant lesion in RCA.
4) Proximal 95% stenosis and mid 90% stenosis in the SVG to the OM (Figure 1, Figure 2)
2) Patent LIMA to LAD with good antegrade flow into the distal LAD.
3) No significant lesion in RCA.
4) Proximal 95% stenosis and mid 90% stenosis in the SVG to the OM (Figure 1, Figure 2)
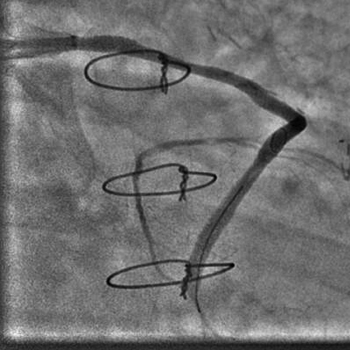
Procedure
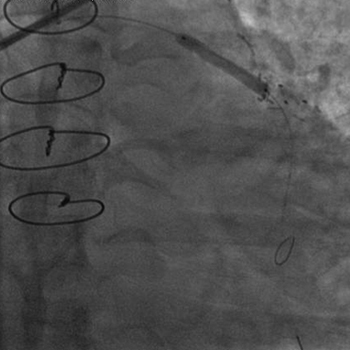
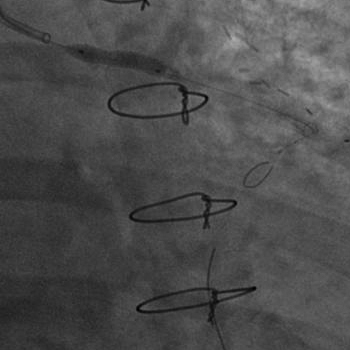
The patient was advised to undergo PCI to SVG to LCx (OM). But she was initially reluctant and was discharged after 5 days of hospitalization. She returned 2 days later with same complaints. The left radial approach was used, and the SVG was cannulated using an Ikari right guiding catheter (6Fr). After a distal protection device (Filter wire EZ, Boston Scientific) was positioned (Figure 3), the mid SVG lesion was directly stented by a 3.5x23mm CC Flex stent (CoCr, Euchatech, Germany) at maximum 16atm (Figure 4). The proximal lesion was stented with a 2.5x15mm BioMatrix DES (Biosensor) at 18atm (Figure 5). The filter wire was removed. Distal TIMI III flow was achieved (Figure 6, Figure 7).
Conclusion(s) / Result(s)
The patient was hemodynamically stable and pain free for the next 2 days until discharge.
Comments/Lessons
For CABG patients, SVG angiography is convenient using a left radial approach rather than a right radial approach. Use of distal protection device is also quite easy through a left radial approach. Ikari guide catheter (Terumo) is getting increasingly popular in our center for transradial PCI.
Gallery


Conflicts of Interest
None
Comments