Use of the Left Judkins Guiding Catheter in an Anomalous Right Coronary Artery with High Anterior Takeoff
by
Fadil Ademaj
January 30, 2012Operator(s)
Fadil Ademaj, Jürgen Stangl, Anil-Martin Sinha
Affiliation
Medizinische Klinik für Kardiologie, Pulmologie und Intensivmedizin
Facility / Institute
Sana Klinikum Hof, Hof, Germany
Clinical History
An 74-year-old gentelman was referred for progressive chest discomfort of 2 weeks duration and syncopal episodes on the admission day. The electrocardiogram (ECG) showed sinus bradycardia with a heart rate of 35 beats per minute, a left axis deviation, and ST depression in II, III, aVF, and V3-V6. Echocardiography demonstrated normal left ventricular function with an ejection fraction of 60% and infero-posterior hypokensia. Laboratory tests did not showed any elevated troponin or MB-CK.
Angiography
1) LAD: 75% stenosis at the proximal segment and 60% stenosis at the distal segment.
2) RCA: Multiple attempts with many different diagnostic catheters (JR4, WRP, AL1, MP1, AR2) failed to engage the RCA in its usual position, and nonselective ascending aortography could not accurately identify the origin of the right coronary artery too.
2) RCA: Multiple attempts with many different diagnostic catheters (JR4, WRP, AL1, MP1, AR2) failed to engage the RCA in its usual position, and nonselective ascending aortography could not accurately identify the origin of the right coronary artery too.
Procedure
Because of his complaints the operator decided to treat the proximal LAD stenosis. A 6Fr EBU 4.0(Launcher, Medtronic, Minneapolis MN, USA) guiding catheter was chosen to engage the LCA. The lesion was easily navigated with 0.014-inch Galeo F guidewire (Biotronic, Berlin, Germany). A 3.5x12mm BMS Integrity (Medtronic, Minneapolis MN, USA) was deployed with an excellent angiographic result with TIMI-3 flow and a myocardial blush grade (MBG) 3.
A positive stress test with 2mm ST depression in inferior leads was found even after a succesful stenting of the proximal LAD.
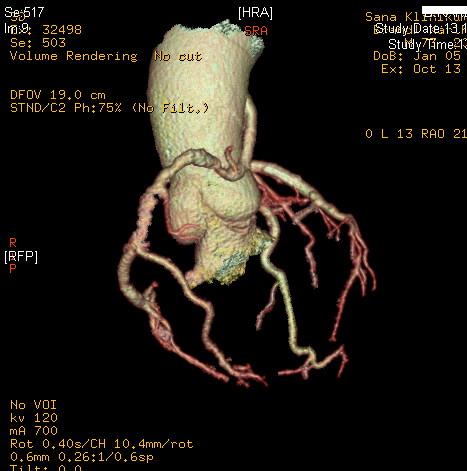
Multislice computed tomography (MSCT) was performed to observe the origin of the RCA that showed a high and anterior take-off anomaly with a significant stenosis at the middle segment.(Figure 1) A very easy cannulation with avery good support was possible only using a 6Fr Judkins left 4 diagnostic and then guiding catheter (Launcher Medtronic, Minneapolis MN, USA) (Figure 2). The RCA lesion was easily navigated with a with 0.014-inch Galeo F guidewire (Biotronic, Berlin, Germany). A 4.0x12mm BMS Integrity (Medtronic, Minneapolis MN, USA) was deployed with an excellent angiographic result.
A positive stress test with 2mm ST depression in inferior leads was found even after a succesful stenting of the proximal LAD.
Multislice computed tomography (MSCT) was performed to observe the origin of the RCA that showed a high and anterior take-off anomaly with a significant stenosis at the middle segment.(Figure 1) A very easy cannulation with avery good support was possible only using a 6Fr Judkins left 4 diagnostic and then guiding catheter (Launcher Medtronic, Minneapolis MN, USA) (Figure 2). The RCA lesion was easily navigated with a with 0.014-inch Galeo F guidewire (Biotronic, Berlin, Germany). A 4.0x12mm BMS Integrity (Medtronic, Minneapolis MN, USA) was deployed with an excellent angiographic result.
Conclusion(s) / Result(s)
MSCT was very helpfull not only to identify the anomalous origin of the RCA, but also in our decision to choose an appropriate diagnostic and guiding catheter with an adequate support resulting in a very succesfull intervention.
Comments/Lessons
We present a case with a rare anomalous origin of the RCA that originates from the upper anterior wall of the ascending aorta. Anomalous origin of the RCA is a rare finding (1). Anomalous origin of coronary arteries has been reported as a cause of angina pectoris, arrhythmia, syncope, and fatal myocardial infarction. Its incidence ranges from 0.61% to 1.3% (2). Coronary anomalies cause up to 17% of deaths in athletes and are associated with 12% of sport-related deaths in 14- to 40-year-old individuals (3). Furthermore, anomalous origination of a coronary artery from the opposite sinus is related to sudden death as reported in frequently quoted autopsy reports (4). MSCT has been shown to be an accurate means of diagnosing coronary anomalies (5, 6).
Gallery

Conflicts of Interest
None
Comments