‘Accelerated Atherosclerosis’ Not Uncommon in Arteries of Young People
Autopsy data from PDAY suggest faster and more dramatic disease progression in some individuals, with no clear link to traditional risk factors.

Postmortem evaluation of coronary arteries from more than 2,600 individuals who died of noncardiac causes before age 35 has identified what appears to be a unique subset whose disease progressed faster and further than would be expected, independent of traditional risk factors.
Understanding what drives the development of atherosclerosis in these young people could lead to improved screening methods, researchers led by Trajen Head, PhD (University of Miami Miller School of Medicine, FL), say. To take a closer look, they used data from the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study.
PDAY was conducted in the mid-1990s, focusing on men and women ages 15 to 34 who had died of accidents, suicides, or homicides. All were in good health, without comorbidities like cancer, overt heart disease, or diabetes.
Pascal J. Goldschmidt-Clermont, MD (University of Miami Miller School of Medicine), senior author of the new analysis published online November 13, 2018, in American Heart Journal, told TCTMD that “it’s important for physicians to be aware that there is a population of patients that seem to be at much higher risk for developing coronary artery disease than the general population.”
“The fact that there is plaque in the coronary arteries at a young age in a sizeable proportion of the population, that to me is the most interesting finding,” said Ron Blankstein, MD (Brigham and Women’s Hospital, Boston, MA), whose own research has shown today’s risk-prediction tools can overlook younger patients apt to experience MI.
Here, he added, what constitutes “young” differs from what has come before. “We’ve actually never done big studies in cardiology ever on people of this age, whether it’s by invasive or noninvasive imaging looking at plaque or by looking at whether different therapies work,” Blankstein said, pointing out that the new cholesterol guidelines released last week emphasize aggressive lifestyle management for patients ages 20 to 39.
What’s less clear is how all this relates to risk factors, he commented to TCTMD. The paper doesn’t contain information on family history of premature coronary heart disease, for example, so it’s possible some factors known to influence atherosclerosis slipped under the radar.
It’s important for physicians to be aware that there is a population of patients that seem to be at much higher risk for developing coronary artery disease than the general population. Pascal J. Goldschmidt-Clermont
Head and colleagues combined data on the number of raised coronary lesions in each individual with information on traditional risk factors for coronary heart disease, such as high cholesterol and body mass index. The idea was to identify which of these risk factors might account for disease progression.
To separate the study cohort into low- and high-growth subgroups, the researchers employed a two-group Poisson mixture model. Around 13% of individuals had “accelerated coronary atherosclerosis despite their young age,” Head et al report, noting that “only age was a significant contributing factor to the observed coronary lesion burden.”
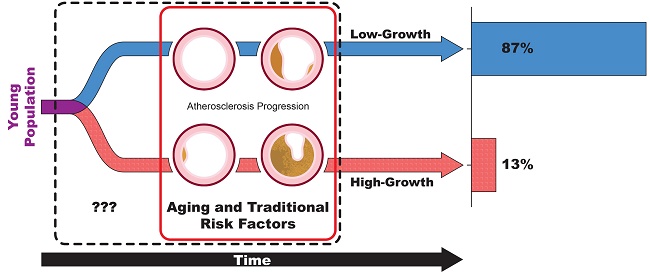
Among young people who died of noncardiac death, 13% had substantially more coronary atheromas that the rest of the population. Traditional risk factors could not account for the excess coronary lesions.
The growth rate in that group was 22 times faster than what was seen in the low-growth group, Goldschmidt-Clermont noted to TCTMD. In the low-growth subset, by around age 24, only one in 10 people had a raised lesion. But in the high-growth subset, each person on average had two lesions—"so a very, very different susceptibility for developing these lesions,” he said.
Aiming for Early Identification
“What’s important to realize is 80% of sudden cardiac deaths are due to atherosclerosis in the coronary arteries,” Goldschmidt-Clermont said, noting that these people have many more lesions than what’s typically seen with slow, continuous development of disease. It’s possible that the accelerated atherosclerosis of the sort seen here precedes sudden cardiac death, he suggested.
“Our results strongly invite that efforts be made to screen for this putative high-risk subpopulation prospectively at as young an age as possible–beyond what is currently recommended for the general population of children and young adults,” the researchers conclude. “Identification of these individuals at risk early could have a tremendous effect on disease prevention and on avoiding deadly outcomes, through more efficient disease management and treatment.”
Blankstein questioned whether the word “accelerated” is suitable. “To me, accelerated means that you’re taking someone and imaging their coronary arteries and looking at how much plaque they have today, and then you repeat it later and you see what the rate of growth is—that’s acceleration,” he observed. “This obviously isn’t what happened here. These people only die once and you take a [snapshot].”
In theory, certain individuals could be having faster growth, but it’s difficult to tell what’s truly happening over time, he explained.
Still, both Blankstein and Goldschmidt-Clermont stressed that the best approach for now is prevention through a healthy lifestyle that involves exercise, a good diet, and avoidance of risk factors like smoking and drug abuse. “People think ‘I don’t have to worry about coronary disease until I’m in my 40s or 50s,’ and folks in their 20s think they’re invincible and they can do whatever they want. . . . This is a disease that develops over a long period of time, and it starts in your teens, if not earlier perhaps, in some people,” Blankstein emphasized.
Photo Credit: Pascal J. Goldschmidt-Clermont, MD

Caitlin E. Cox is Executive Editor of TCTMD and Associate Director, Editorial Content at the Cardiovascular Research Foundation. She produces the…
Read Full BioSources
Head T, Henn L, Andreev VP, et al. Accelerated coronary atherosclerosis not explained by traditional risk factors in thirteen percent of young individuals. Am Heart J. 2018;Epub ahead of print.
Disclosures
- The paper contained no information on potential conflicts of interest.
- Blankstein reports no relevant conflicts of interest.
Arreka Jorkman
Arreka Jorkman