NOTION-3: PCI Before TAVI Lowers MACE Risks in Patients With Significant CAD
There was a reduction in MACE with PCI before TAVI, but that doesn’t mean revascularization should be the norm, say experts.

LONDON, England—Patients with stable coronary artery disease and severe aortic stenosis fare significantly better over the long term if revascularized with PCI before TAVI than if they are treated with a conservative strategy of guideline-directed medical therapy before the aortic-valve intervention, according to results of a new randomized trial.
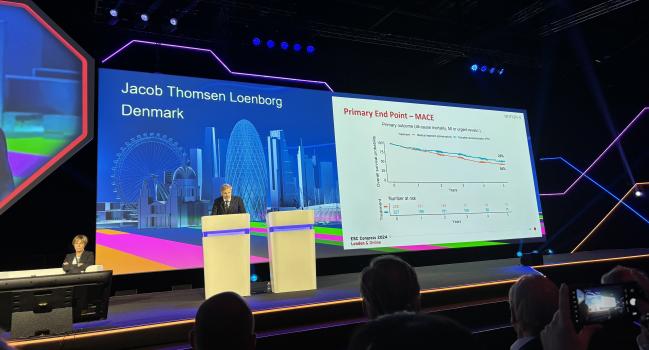
The NOTION-3 study, which was presented today as a Hot Line at the European Society of Cardiology Congress 2024 and published simultaneously in the New England Journal of Medicine, showed that coronary revascularization before TAVI resulted in a 29% lower relative risk of all-cause mortality, MI, or urgent revascularization after a median of 2 years when compared with medical therapy before TAVI.
Jacob Thomsen Lønborg, MD, PhD (Copenhagen University Hospital—Rigshospitalet, Denmark), said that based on their findings, PCI prior to TAVI should be done for all patients with significant coronary artery disease.

“That would be our recommendation: that the standard of care would be to do PCI,” Lønborg told TCTMD. “Of course, as a physician, you need to individualize treatment. You need to look at your patient and take into account their risk of bleeding, age, comorbidities, symptoms, and the complexity of their coronary artery disease and the procedures. Those are the things that should be considered.”
That would be our recommendation: that the standard of care would be to do PCI. Jacob Thomsen Lønborg
Rishi Puri, MD, PhD (Cleveland Clinic, OH), senior investigator of a large observational analysis showing that residual obstructive CAD—even significant left main and triple-vessel disease—could be safely left alone in patients undergoing TAVI for severe aortic stenosis, urged interventional cardiologists to interpret NOTION-3 cautiously. He disagrees with any interpretation that this trial is a green light to revascularize all significant coronary lesions prior to TAVI.
“In my humble opinion, that’s not what NOTION-3 tells us, nor that is what many of us practice as both coronary and TAVI operators,” Puri told TCTMD.
While there was a significant reduction in the primary endpoint with PCI, event curves didn’t separate until roughly 1 year, which gives clinicians sufficient time to get to the bottom of a patient’s symptoms and be selective with what patients and lesions you want to treat, he said.
“You perform TAVR, and you’re left with residual obstructive coronary artery disease, and whether it's single vessel disease or left main/multivessel disease, what do you do about it?” asked Puri. “What NOTION tells you is that you have around 1 year after TAVR before patients start to accrue events, mostly revascularization. The patients that were problematic, the ones that ended up having events, were more likely to be those with at least a 90% narrowing. So, you have time to closely follow these patients and really ask them, ‘Hey, do you have any residual shortness of breath or are you getting some chest discomfort, despite a successful TAVI procedure, that antianginals aren’t helping with?’”
Shamir Mehta, MD (Hamilton Health Sciences/Population Health Research Institute, Hamilton, Canada), the discussant following Lønborg’s presentation, called NOTION-3 a solid, well-conducted clinical trial. Like Puri, though, he noted that the benefit of PCI prior to TAVI was mainly due to a reduction in the need for coronary revascularization.
“So, that will pose the question, why not tailor PCI for the symptomatic patients and do [PCI] after TAVR? And that would save a large amount of unnecessary PCI,” said Mehta, adding that it would also limit patient exposure to dual antiplatelet therapy and accompanying bleeding risks.
PCI vs Medical Therapy
There aren’t clear US or European recommendations for the treatment of coronary artery disease in patients with symptomatic severe aortic stenosis requiring TAVI. The European Association of Percutaneous Cardiovascular Interventions (EAPCI) recently provided some direction on revascularization in patients with severe aortic stenosis. They recommend PCI prior to TAVI in patients with severe CAD, which is defined as coronary artery stenosis > 70% (or > 50% for proximal segments of the left main coronary artery, particularly if presenting with ACS, angina, or other subocclusive lesions). The timing of PCI should be based on the patient’s anatomy and lesion complexity.
NOTION-3 included 455 patients (median age 82 years; 67% male) with at least one coronary stenosis deemed physiologically significant (fractional flow reserve [FFR] 0.80 or less) or those with a diameter stenosis 90% or greater. Patients were randomized to complete revascularization of all PCI-eligible lesions in coronary arteries that were 2.5 mm in diameter meeting the FFR or angiographic criteria. Those assigned to conservative therapy were treated with aspirin 75 mg once daily as well as clopidogrel 75 mg once daily for 3 months. However, after the publication of POPular-TAVI, the medically managed patients were treated with aspirin monotherapy.
The median time from randomization to TAVI was 34 days for those in the PCI arm and 25 days for those assigned to medical therapy. PCI was performed concomitantly with or shortly after TAVI in 26% of patients. Complete revascularization was achieved in nearly 90% of cases.
Why not tailor PCI for the symptomatic patients and do [PCI] after TAVR? And that would save a large amount of unnecessary PCI. Shamir Mehta
After a median of 2 years, the MACE rate was 26% for those revascularized before TAVI and 36% in those treated conservatively (HR 0.71; 95% CI 0.51-0.99). With respect to secondary endpoints, there was no difference in mortality between treatment arms, but the rate of MI was higher in those managed conservatively (14.0% vs 7.0%; HR 0.54; 95% CI 0.30-0.97) as were rates of urgent revascularization (11.0% vs 2.0%; HR 0.20; 95% 0.08-0.51) and any revascularization (21% vs 3.0%; HR 0.12; 95% CI 0.05-0.27).
In a subgroup analysis, the reduction in MACE was seen only in those with a diameter stenosis 90% or greater.
As to why there was a reduction in MI and need for revascularization with PCI, Lønborg speculated that TAVI “unmasked” the coronary artery disease. “These patients had severe aortic stenosis and they probably would have decreased their physical activity levels,” he said. Once they underwent the valve procedure, and their activity levels picked up again, this could have triggered MI or symptoms requiring revascularization in the group left untreated before TAVI.
In NOTION-3, the risk of bleeding was significantly greater in patients randomized to PCI before TAVI: 28.0% vs 20.0% (HR 1.51; 95% CI 1.03-2.22). Lønborg said they are planning to analyze the data further to identify patients who might be more prone to bleeding, which would allow clinicians to home in avoiding PCI in those at highest risk.
Role of PCI in Stable Patients
Simon Redwood, MBBS (Guy’s and St Thomas’ NHS Foundation Trust, London, England), who led the ACTIVATION trial looking at the risks and benefits of PCI before TAVI, praised the NOTION-3 investigators, calling it a compelling result that should change practice. ACTIVATION, which was presented at PCR London Valves several years back, found the opposite of NOTION-3: performing PCI prior to TAVI in patients with at least one significant coronary stenosis did not lower the risks of death/rehospitalization when compared with patients who weren’t revascularized.
“This is a much more contemporary study,” he told TCTMD. “We had a lot of problems with ACTIVATION. One of them being we designed the trial well over 10 years ago when TAVI was a very different procedure. Vascular complications were much higher—we were using much bigger sheaths and a lot more of it was done under general anesthesia.”
Recruitment into ACTIVATION was slow and investigators eventually ran out of funding. As a result, they ended up with a much smaller trial that was underpowered for clinical endpoints, said Redwood. “The other important thing is that we mandated that patients did not have to have angina,” he said.
This goes against all the bulk of the evidence that we have so far. Rodrigo Bagur
Several years back, Rodrigo Bagur, MD, PhD (Western University/London Health Sciences Centre, Canada), showed there were more vascular complications and higher 30-day mortality with PCI prior to TAVI. Given the prior data, Bagur was skeptical of the NOTION-3.
“This is the first one to show positive results supporting PCI versus a conservative or medical management approach,” he said. “This goes against all the bulk of the evidence that we have so far.”
For Bagur, though, there is still much some uncertainty around the NOTION-3 findings. He highlighted the wide confidence intervals around the primary endpoint and also questioned the 80% reduction in urgent revascularizations, noting that numbers were very small—five events with PCI-treated patients versus 25 in those randomized to conservative treatment. None of the secondary endpoints were adjusted for multiplicity, he added.
Patients with severe aortic valve disease might have chest pain, said Bagur, but the primary symptoms are shortness of breath and fatigue. At their high-volume center, which performs more than 300 TAVIs per year, with many others referred onto to surgery, the majority of patients present with classic symptoms of aortic stenosis, not angina or equivalents, he said. And for the chronic coronary syndrome patient, the bulk of the evidence says to treat them with antianginal medications if they have angina, said Bagur.
Puri agreed.
“If they weren’t having TAVR, in a lot of these patients, you wouldn’t know they had obstructive disease as you may not be performing coronary angiography as a part of the workup,” he said. “All the guidelines for stable coronary artery disease tell us that in the absence of angina [that is] difficult to control with antianginals, what is the indication to stent? There isn’t a strong one.”
To TCTMD, Redwood said their decision to revascularize before PCI hinges on patient symptoms and this may explain the NOTION-3 results.
“The patients that they included were those with significant disease, and if most of them had angina, which they did, then the results make sense,” he said. “We tend to go by symptoms. If the patient doesn’t have angina, unless they’ve got a significant left-main stem stenosis or equivalent left main, we will not treat them. We will do their TAVI, but we will generally put in a valve which will allow easy access to the coronary arteries. If they develop angina once they’re more active after having TAVI, we’d bring them back and do the PCI.”
He noted that those treated with medical therapy in NOTION-3 had a higher risk of urgent revascularization, but said that typically isn’t their experience. If patients with significant CAD without symptoms are treated with TAVI first, Redwood said they are closely followed after discharge.
During his presentation, Mehta hailed NOTION-3 as a solid step in the right direction for providing clinicians with evidence to guide practice. It’s not the end of the story, though. The COMPLETE-TAVR trial is ongoing, a 4,000-patient study comparing staged complete revascularization versus medical therapy in patients with at least one coronary lesion who are scheduled for TAVI.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Lønborg J, Jabbari R, Sabbah M, et al. PCI in patients undergoing transcatheter aortic-valve implantation.N Engl J Med. 2024;Epub ahead of print
Disclosures
- Lønborg reports grants from Abbott Medical Optics and grants/speakers fees Boston Scientific.
- Mehta reports no relevant conflicts of interest.
Related News



Comments