Preventive VT Ablation Before ICD Helps High-risk Ischemic Cardiomyopathy Patients
If the findings are borne out in a more-definitive trial, it “could have a pretty major impact,” one expert says.

BERLIN, Germany—Performing ventricular tachycardia (VT) ablation before placement of a primary prevention implantable cardioverter-defibrillator (ICD) had a clinical benefit in a selected group of ischemic cardiomyopathy patients at high risk for ventricular arrhythmias, results from the randomized PREVENTIVE VT trial show.
The study included patients with a reduced ejection fraction and a chronic total occlusion (CTO) in an infarct-related artery who were not eligible for revascularization. Those randomized to VT ablation before ICD implantation had a significantly lower rate of ICD therapy or hospitalization related to ventricular arrhythmias than those who received a defibrillator without ablation (16.7% vs 43.3%).
David Žižek, MD, PhD (University Medical Centre Ljubljana, Slovenia), who reported the data here at the European Heart Rhythm Association Congress 2024, stressed the importance of identifying patients at high risk for ventricular arrhythmias for whom VT ablation as a primary prevention strategy, with its potential risks, might make sense.
These results, from a 60-patient trial, “warrant future adequately powered studies that explore not only efficient and safer catheter ablation technologies, but also newer imaging modalities to potentially establish this concept in the clinical practice,” he said.
The PREVENTIVE VT Trial
Although ICDs have proven to be lifesaving, appropriate shocks have been associated with reduced quality of life and adverse clinical outcomes. There is a question about the utility of performing VT substrate ablation, and when it should be done, with some data showing that performing the intervention in patients with recorded ventricular arrhythmias before ICD implantation lowers arrhythmia recurrence, Žižek said.
Evidence is mixed in terms of the impact of such an approach on clinical outcomes, but prior studies have demonstrated that deferring ablation is associated with worse prognosis, lower success rates, and increased procedural complications.
This raises the question, Žižek indicated, of whether substrate ablation may be useful as a primary prevention strategy.
Before testing the concept in a randomized trial, it was important to identify the right patient population, he said, noting that patients with a CTO in an infarcted area who are not deemed suitable for revascularization have a high rate of ventricular arrhythmias.
Thus, for the PREVENTIVE VT trial, investigators across four Slovenian centers enrolled 60 patients (mean age about 67 years; 92% men) with ischemic cardiomyopathy, an infarct-related CTO, and a primary prevention ICD indication. Mean LVEF was about 35%. Nearly half (48%) had a history of symptomatic MI, 43% a history of PCI, and 8% a history of surgical revascularization.
Those randomized to VT ablation underwent the procedure before ICD implantation, with the goal of eliminating all abnormal electrograms after high-density remapping and VT noninducibility.
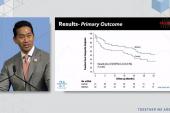
The primary endpoint was the time to ICD therapy or unplanned ventricular arrhythmia-related hospitalization, and through a mean follow-up of 44.7 months, that risk was reduced among patients who underwent ablation before receiving their ICD (adjusted HR 0.32; 95% CI 0.11-0.91).
There was a nonsignificant trend toward less ICD therapy (16.7% vs 40%; HR 0.35; 95% CI 0.12-1.02). All nine unplanned hospitalizations for symptomatic ventricular arrhythmias occurred in patients in the ICD-alone group.
Unplanned cardiac hospital admissions (including those for ventricular arrhythmias and for heart failure) were less frequent after ablation plus ICD implantation (13.3% vs 53.3%; HR 0.22; 95% CI 0.07-0.68). There were six cases of electrical storm, all in the ICD-alone group.
No significant differences between trial arms were seen in heart failure hospitalization, cardiovascular death, or all-cause death. Safety of ablation was reasonable, Žižek said, reporting two ablation-related complications (6.6%)—one complete AV block that required implantation of a cardiac resynchronization therapy-defibrillator, and one ischemic stroke that resolved without consequences.
Promise of Precision Medicine
Serving as the discussant after Žižek’s presentation, William Stevenson, MD (Vanderbilt University Medical Center, Nashville, TN), pointed out that the concept of performing catheter ablation in a patient receiving an ICD was tested in the SMASH VT trial, with results reported in 2007. The trial showed that in patients with a prior MI who were receiving an ICD, performing VT substrate ablation reduced the arrhythmia without influencing mortality. Though this was a landmark trial, it didn’t change practice, Stevenson said.
He questioned whether PREVENTIVE VT, which has now demonstrated reductions in VT and hospitalizations for arrhythmia using a similar strategy, will sway how clinicians are managing these patients.
“For that to be clinically applicable, it has to be extremely safe,” Stevenson said, highlighting the two adverse events in the ablation arm of this small trial. AV block is to be expected in patients with VT and septal substrate, he said, adding, however, that “the stroke is perhaps a little more worrisome. But again, one event in a small trial.”
He called for further research into the usefulness of this strategy. “But I’m particularly enthusiastic about this because it’s an example of, I think, where our field should be going, which is in precision medicine—identifying the right treatment for the right patient,” Stevenson said. “Here is a very specific subgroup of patients at high risk for VT—someone with an infarct with an occluded infarct artery—in whom there’s an opportunity to make a difference.”
Speaking with TCTMD, Stevenson pointed to the reduction in hospitalizations as a key component of the trial. “Although there’s not a signal that it improves mortality, the study was underpowered for that, but it had a significant effect to reduce hospitalizations and that could have a pretty major impact,” he said.
The approach studied here would have been more challenging 10 to 20 years ago, Stevenson noted. “The reason this is even worth considering is that there have been substantial technical advances in catheter ablation and mapping that make this doable for most practicing electrophysiologists.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Žižek D. Impact of preventive substrate catheter ablation on implantable cardioverter-defibrillator interventions in patients with ischemic cardiomyopathy and infarct-related coronary chronic total occlusion: the PREVENTIVE VT randomized multicenter trial. Presented at: EHRA 2024. April 8, 2024. Berlin, Germany.
Disclosures
- The study was supported by an institutional research grant from University Medical Centre Ljubljana.
- Žižek reports proctoring fees and speaking honoraria from Medtronic, Biotronik Abbott, and Boston Scientific.
Related News


Comments