TCAR Use Growing for Carotid Stenosis as Positive Data Continue to Accumulate
The procedure—a hybrid of surgical and endovascular techniques—offers low stroke rates and a short learning curve.

Transcarotid artery revascularization (TCAR), which pulls in both surgical and endovascular techniques, is being rapidly adopted in the United States for the treatment of high-risk patients with extracranial carotid artery stenosis. Now, emerging real-world data suggest that it provides outcomes at least as good as—and possibly better than—other options.
Three presentations at the 2019 Society for Vascular Surgery (SVS) Vascular Annual Meeting held last week in National Harbor, MD, showed that even in the hands of operators without prior experience with TCAR, the procedure provides rates of stroke, death, and MI that are low and comparable to those seen with carotid endarterectomy (CEA) and better than those obtained with traditional transfemoral stenting.
In the ROADSTER 2 trial, a US Food and Drug Administration-mandated postapproval study, TCAR with the Enroute transcarotid neuroprotection and stent system (Silk Road Medical) provided a 30-day stroke/death/MI rate of 1.7%, lower than the rate seen in the earlier ROADSTER 1 trial supporting FDA approval of the system (3.0%) and in the CEA arm of the CREST trial (4.5%). Four out of five operators in ROADSTER 2 were new to the procedure.
Favorable data also came from two studies out of the TCAR Surveillance Project, part of the SVS Vascular Quality Initiative. One showed that compared with CEA, TCAR was associated with lower in-hospital risks of MI, stroke/death/MI, and cranial nerve injury and lower 1-year risks of death and stroke. The other demonstrated superior outcomes with TCAR versus transfemoral stenting in patients 80 and older and similar outcomes with TCAR and CEA regardless of age.
CEA remains the gold standard, according to Mahmoud Malas, MD (University of California, San Diego), who was involved in all three analyses, but the new findings support the viability of TCAR as a safe and effective third revascularization option for patients with carotid stenosis.
Vikram Kashyap, MD (University Hospitals Cleveland Medical Center, OH), who presented ROADSTER 2, said the results are “very promising” but indicated that there’s more work to be done to evaluate TCAR.
I think it’s too early to say a whole lot about that based on registry data, but I do think it’d be worth looking into further. Nicholas Osborne
“I think the next step is a prospective randomized trial,” he told TCTMD, adding, “I think the narrative has changed a bit. A few years ago we were thinking that that prospective trial would be TCAR versus transfemoral carotid artery stenting, and perhaps we’re at a stage where we can consider TCAR versus carotid endarterectomy.”
Commenting for TCTMD, vascular surgeon Nicholas Osborne, MD (University of Michigan and VA Ann Arbor Healthcare System), who was not involved in the studies, said the real-world experience “continues to demonstrate the effectiveness of TCAR. I think it’s encouraging data and it’s exciting to see that the data continue to show a benefit outside of the trials.”
ROADSTER 2
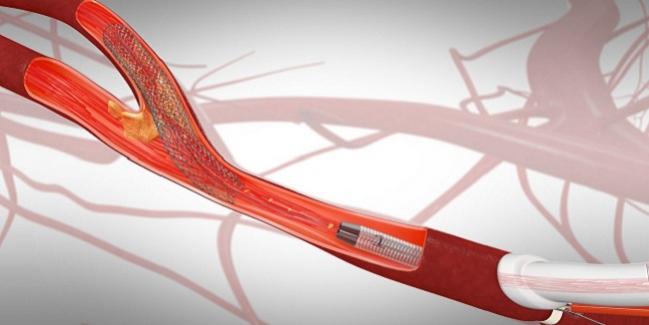
TCAR using the Enroute system incorporates both surgical and endovascular elements. After making a small incision at the base of the neck, operators place a sheath in the carotid artery, through which neuroprotection is established by reversing the flow of blood. That blood is filtered externally and then returned through the femoral vein. A stent is delivered via the transcarotid approach while the blood flow is reversed.
“The main benefits of this procedure,” Malas explained, “are avoiding the atherosclerotic and often tortuous aortic arch; providing a CEA-like protection by clamping the common carotid artery; performing all parts of the procedure under the protection of robust dynamic flow reversal; and easing the intervention by having direct access with shorter wires, catheters, and stent delivery system.”
The procedure is fairly straightforward to learn, and the learning curve is short, Kashyap said.
The FDA approved the Enroute neuroprotection and stent systems in 2015 based on the results of the ROADSTER 1 investigational device exemption trial, in which TCAR provided clinical outcomes that compared favorably with those obtained with CEA in the CREST trial.
As a condition of approval, the FDA mandated a postapproval study, which became ROADSTER 2. Kashyap presented the final results of the study, which involved 632 symptomatic and asymptomatic patients treated at 42 centers.
The primary endpoint was procedural success at 30 days, defined as technical success in the absence of stroke, death, or MI. The success rate was 97.9%, exceeding the a priori threshold of 85.0% (P < 0.0001).
In the first 30 days of follow-up, six patients had an MI, four patients had a stroke, and one died of a ruptured abdominal aortic aneurysm. There were no neurological or cardiac deaths. The stroke/death rate was 0.8% overall, and came in below 1% in both asymptomatic and symptomatic patients (0.9% and 0.6%, respectively). For comparison, the 30-day stroke/death rate in the CEA arm of CREST was 2.6%.
Excellent outcomes also were seen in other high-risk groups, including women and elderly patients, Kashyap reported.
He underscored that 80% of operators in ROADSTER 2 were new to TCAR. “Despite this novice group, they achieved outcomes that were broadly similar, perhaps even a bit better, than ROADSTER 1,” he said.
TCAR Surveillance Project
Speaking with TCTMD, Malas discussed two analyses out of the TCAR Surveillance Project, one that he presented at the SVS meeting and another presented by Hanaa Dakour-Aridi, MD (University of California, San Diego).
Updating a prior analysis that showed similar in-hospital and 30-day outcomes with TCAR and CEA but less cranial nerve injury with TCAR, the investigators examined surveillance data on 5,716 TCARs and 44,442 CEAs performed between September 2016 and May 2019. During that time span, there was a rapid increase in the number of TCAR procedures performed.
After propensity-score matching, TCAR was associated with lower in-hospital risks of MI (OR 0.41; 95% CI 0.26-0.66), stroke/death/MI (OR 0.65; 95% CI 0.50-0.84), cranial nerve injury (OR 0.13; 95% CI 0.07-0.22), postprocedural hypertension (OR 0.64; 95% CI 0.57-0.71), non-home discharge (OR 0.75; 95% CI 0.64-0.87), a hospital stay longer than 1 day (OR 0.74; 95% CI 0.68-0.80), and a higher risk of postprocedural hypotension (OR 1.66; 95% CI 1.47-1.87), compared with CEA. Differences in MI and stroke/death/MI were seen in both asymptomatic and symptomatic patients.
An advantage for TCAR in terms of mortality emerged by 30 days. The unadjusted rate was 0.7% with both TCAR and CEA, but after adjustment, risk was lower with TCAR (OR 0.66; 95% CI 0.46-0.95). At 1 year, the unadjusted mortality rate was 3.3% with CEA and 3.4% with TCAR, but risk was lower with TCAR after propensity-score matching (HR 0.77; 95% CI 0.62-0.96).
Asked about how much weight to put into the observed mortality difference, Malas said it should be taken with grain of salt because of the nonrandomized nature of the analysis. It could be, however, that the lower rate of postoperative MI—which has been tied to increased mortality—following TCAR versus CEA is translating into improved survival.
Malas said, “I believe this study provides strong evidence on the safety and effectiveness of TCAR. Larger studies with longer follow-up are needed to confirm our findings and evaluate the indication of this procedure in normal-risk patients.”
Vascular surgeons not involved in the analyses were skeptical of the mortality difference.
“I personally wouldn’t read much into that finding,” Osborne said, stating that it was likely related to differences between patient populations that were not fully captured. “I think it’s too early to say a whole lot about that based on registry data, but I do think it’d be worth looking into further.”
Similarly, Brajesh Lal, MD (University of Maryland Medical Center, Baltimore, MD), said it’s “very, very difficult to interpret that and to rely on it. This is registry data, and I would be very careful in overinterpreting comparisons.”
Additional real-world registry data exploring the impact of age on the outcomes of revascularization by TCAR, CEA, or transfemoral stenting were presented by Dakour-Aridi. It was initially thought that stenting would have a particular benefit in older patients because it is less invasive than surgery, but several studies have shown that the risks of stenting increase with age, leading to a greater advantage for CEA. That seems to be related to the increased prevalence of severe aortic arch and target-lesion calcification and ulceration, which raise the risk of plaque-degree embolization while maneuvering catheters, in older patients. Because TCAR avoids the need to cross the arch, it may cut down on embolic risks.
To look at the effect of age, the researchers examined carotid procedures performed between 2015 and November 2018 and catalogued in the Vascular Quality Initiative databases. The analysis included 3,152 TCARs, 10,381 transfemoral stenting procedures, and 61,650 CEAs.
In-hospital outcomes were mostly similar with TCAR and transfemoral stenting in patients younger than 80, with the exception of a lower rate of death with TCAR in patients ages 71 to 79 (0.3% vs 1.0%; P = 0.04). In patients 80 and older, however, TCAR carried lower rates of death (0.7% vs 2.5%), ipsilateral stroke (0.9% vs 4.2%), stroke (1.0% vs 4.7%), stroke/TIA (1.7% vs 5.4%), stroke/death (1.5% vs 4.6%), and stroke/death/MI (2.5% vs 5.3%; P < 0.01 for all). The TCAR advantage for stroke, stroke/TIA, stroke/death, and stroke/death/MI persisted after adjustment.
In contrast, when comparing in-hospital outcomes for TCAR versus CEA, there were no differences in any age group before or after adjustment.
Choosing the Best Procedure
In the absence of head-to-head trials of TCAR versus either transfemoral stenting or CEA—and with no concrete plans to perform them—the question then becomes: how do you choose the right procedure for the right patient?
Lal said the decision involves considerations of anatomical, patient-related, and lesion-related factors. For example, operators have learned over the years that older patients don’t do as well with transfemoral stenting versus CEA and that patients with radiation-induced stenoses or lesions that are very high in the carotid artery don’t fare as well with CEA as with transfemoral stenting.
In addition, the choice of procedure might be influenced by the skill set of the physician to whom a patient has been referred. All vascular surgeons are adept at performing CEA, but fewer are comfortable performing transfemoral stenting and an even smaller—but rapidly expanding—proportion are trained to do TCAR, Lal said.
Kashyap noted that anatomical factors that would preclude TCAR are a distance between the clavicle and the carotid bifurcation—the “landing zone”—of less than 5 cm and severe local changes in the neck due to radiation or a stoma from a prior tracheostomy.
Malas noted that severe disease in the proximal common carotid artery or a deep carotid artery would also push the decision away from TCAR.
But if a stent is indicated and there are no anatomical contraindications, “TCAR is definitely the way to go,” Malas said.
The technology seems to be extremely promising, this approach seems to be extremely promising, and the learning curve does not appear to be a big one. Brajesh Lal
Osborne agreed, noting that TCAR has displaced transfemoral stenting in nearly all of his cases in which a stent is used. “At this point, I think transcarotid revascularization really will surpass transfemoral stenting as the minimally invasive approach to treating carotid artery disease, except in the instances where we can’t physically do it because of anatomic considerations that preclude transcarotid stenting,” he said.
When deciding between TCAR and CEA, Osborne said, “that’s a decision that really should be made with the patient and the provider together, because I think that this data reinforces that it seems like both are good, safe options and both have very similar risk profiles” in terms of major adverse clinical outcomes, with a lower risk of cranial nerve injury with TCAR.
Therefore, patient preference will likely play a major role when choosing between CEA and TCAR. “I think it’s important that we keep them both in our skill set to be able to offer to patients so that we can give them really what I would consider more patient-centered care,” Osborne said.
Outlook of TCAR
Hovering over this entire discussion is the issue of whether revascularization is even needed in the modern era of medical therapy, a question being explored in the parallel trials of CREST-2—one comparing CEA plus medical therapy to medical therapy alone and one comparing transfemoral stenting plus medical therapy to medical therapy alone. CREST-2 is enrolling only asymptomatic patients.
Lal, a co-principal investigator of CREST-2, said leadership considered whether TCAR should be allowed in the trial but decided to not allow it, both because it’s still a relatively new technology and the safety has not been fully elucidated and because it doesn’t fit neatly into either the surgical or the stenting part of the trial.
Thus, the field will have to wait for a randomized trial of TCAR, which is needed, Lal said.
“The technology seems to be extremely promising, this approach seems to be extremely promising, and the learning curve does not appear to be a big one. And at the very least and based on the currently available data, it shows that it’s not inferior to either of the two procedures that are available, and registry data seems to show the same thing and perhaps a signal that it may even be a little better,” Lal said.
“By the same token, because physicians are beginning to use this in an extremely accelerated fashion, it is becoming more and more important that these procedures—at the very least TCAR—undergo a randomized trial comparison,” he added. “Without that no one will be able to make a data-driven, informed decision and provide an informed answer to . . . which patient should get what.”
Ultimately, the rapid adoption of TCAR will continue and it will be commonplace for vascular surgeons to offer it, Osborne predicted.
“I do think it’s correct to roll it out in a controlled fashion. I think the company has done a good job of education and preparing providers for how to do this procedure,” he said, adding that SVS and government regulators have done well with introducing TCAR into the market and with tracking outcomes through registries. “It’s a good demonstration of the real-world effectiveness of the technique and the power of registry data to help guide our clinical care,” Osborne concluded.
Photo Credit: Silk Road Medical

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Dakour-Aridi H, Kashyap VS, Wang GJ, et al. Age and outcomes after transcarotid artery revascularization, transfemoral carotid artery stenting, and carotid endarterectomy. Presented at: SVS VAM 2019. June 12, 2019. National Harbor, MD.
Malas MB, Dakour-Aridi H, Kashyap VS, et al. Outcomes of transcarotid revascularization with dynamic flow reversal versus carotid endarterectomy in the Transcarotid Revascularization Surveillance project. Presented at: SVS VAM 2019. June 13, 2019. National Harbor, MD.
Kashyap VS, Schneider PA. Transcarotid artery stenting in patients with significant carotid artery disease: ROADSTER 2 trial results. Presented at: SVS VAM 2019. June 15, 2019. National Harbor, MD.
Disclosures
- Malas reports performing contracted research for and serving as a proctor for Silk Road Medical.
- Kashyap, Dakour-Aridi, and Osborne report no relevant conflicts of interest.
Comments