Athletes Have Telltale CMR Markers of Damage Post-COVID-19, but Clinical Significance Unclear
The small series will fuel the contentious debate over the lasting cardiac effects, but everyone agrees: more data are needed.

Four of 26 competitive athletes at Ohio State University who recovered from non-severe COVID-19 had cardiac MR (CMR) imaging evidence of myocarditis and an additional eight patients had signs of prior myocardial injury, researchers report in a research letter today. They say their findings should inform the debate over the kind of follow-up warranted before athletes return to sport; the data will also no doubt fuel the ongoing discussions over how, and how long, COVID-19 can impact the heart.

“Cardiac magnetic resonance imaging has the potential to identify a high-risk cohort for adverse outcomes and may, importantly, risk stratify athletes for safe participation because CMR mapping techniques have a high negative predictive value to rule out myocarditis,” write Saurabh Rajpal, MD (Ohio State University, Columbus), and colleagues in an early online publication of JAMA Cardiology.
Speaking with TCTMD, Rajpal said, “we were expecting to find something” in their series based on other CMR studies published in the last few months. “We knew from the COVID-19 literature that was coming out that there was possible cardiac involvement, so we were looking for a test that would be safe so that athletes could return to competition and play. In addition to clinical exam, electrocardiography, and echocardiography, CMR would provide us with data about cardiac inflammation. None of the other tests could do that.”
What’s not clear, Rajpal continued, is whether the findings, which point to an inflammatory phase of myocarditis, ultimately resolve or produce lasting damage.
Playing With Heart
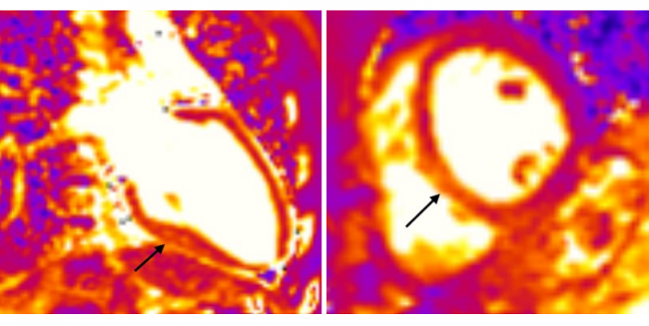
Athletes in this study had a mean age of 19.5 years, were predominately men (58%), and came from various sports: football, soccer, lacrosse, basketball, and track. Evidence of myocarditis on CMR was based on the presence of two main features: myocardial edema by elevated T2 signal and myocardial injury by presence of nonischemic late gadolinium enhancement (LGE).
Rajpal and colleagues point out that a recent expert consensus document on returning to competitive sport recommends 2 weeks of convalescence but states that diagnostic cardiac tests are not warranted following an asymptomatic course, whereas an electrocardiogram and transthoracic echocardiogram may be advisable following a symptomatic infection. “Emerging knowledge and CMR observations question this recommendation,” Rajpal et al write.
In their Ohio State series, only 12 of the 26 screened athletes had any COVID-19 symptoms. Of the four—all male—with evidence of myocarditis, two never had any symptoms of COVID-19.
Jonathan H. Kim, MD (Emory University School of Medicine, Atlanta, GA), who the co-authored the recommendations published last May, spoke with TCTMD about the Rajpal paper.
Back in the spring, Kim said, he and his co-authors called their document a “game plan” for returning to sport, in part because they lacked the data to make firmer recommendations as to what tests are needed and when. “I would submit that we still don't have the type of rigorous data to know what the right algorithm is,” Kim told TCTMD. “It's important that we continue to gather these types of data, but there are limitations as well.”
I would submit that we still don't have the type of rigorous data to know what the right algorithm is. Jonathan Kim
“We need to be concerned about COVID-19 and we need to be careful about return to play, but I would be very cautious in terms of taking it the next step in saying that CMR should be widely used for screening,” Kim said. “I don't think this study answers that question.”
Rajpal, to TCTMD, also made the point that the study was small, lacked a control group, and is complicated by the fact that athletes are a group already known to experience unique cardiac effects of high-intensity sport. And he stopped short of saying that CMR should be used more widely in athletes screening.
“How each program decides to manage their patients depends on a lot of things. We had the capability and the resources to do this type of test of athletes, so we did it,” Rajpal said. “Again I think we do need more data to support MRI or not, depending on what the data show, but clearly when we found inflammation in some of those patients that would not have been picked up using the previous protocols. But each program needs to come up with their own plan. Our goal was merely to generate more data.”
CMR in COVID-19
The use of cardiac MR in convalescent COVID-19 and beyond has received a groundswell of attention after studies in the United Kingdom, China, and Germany suggested that the COVID-19 was producing cardiac changes that could be picked up weeks and months after infection, even in patients who never had serious illness. In particular, the paper by Valentina Puntmann, MD, PhD (University Hospital Frankfurt, Germany), and colleagues made headlines around the world after documenting abnormal CMR findings in 78% of patients scanned, despite the fact that 67% were never hospitalized. The paper got even more attention after some of its numbers were picked apart on Twitter, prompting a rapid correction by Puntmann and senior author Eike Nagel, MD (University Hospital Frankfurt, Germany), accompanied by a letter of support by the journal editors.
Commenting on the Ohio State series for TCTMD, Puntmann and Nagel called the study “important,” saying that it adds “significant information on the discussion about myocarditis” in the setting of COVID-19.
“In general, the findings confirm our initial observations with a similar range of cardiac abnormalities (more LGE, slightly less T2) in a healthier population—younger, less symptoms, less comorbidities—than our cohort,” they said in an email. “We believe that there are three important messages. First, people recovered from COVID-19 have a high prevalence of cardiac involvement; second, healthier populations with less symptoms—as seen now as the main group of new infections—have less cardiac damage; and third, cardiac MRI is an important tool for assessing cardiac involvement, which is not detected by echocardiography.”
Puntmann, Nagel, Rajpal, and Kim all agreed that this is an active area of investigation in need of more standardization for the CMR approach and more data, not only in COVID-19 survivors but also in control populations. Kim pointed out that very little is known about what MRI findings would look like in a person who’d recovered, for example, from another type of respiratory virus. Also, he said, nearly half of the patients in the Rajpal series had LGE, but it’s impossible to know what the clinical significance of that might be.
Rajpal noted that they are continuing to enrol more patients for CMR screening and plan to rescan patients already tested. “In the next iteration of the paper, we will include that data because we hope that [CMR evidence of myocardial inflammation] improves, that it is acute, because in other viral myocarditis papers it has been shown to improve, if not in everyone, than at least in the majority of patients, he said.
Photo Credit: Saurabh Rajpal

Shelley Wood was the Editor-in-Chief of TCTMD and the Editorial Director at the Cardiovascular Research Foundation (CRF) from October 2015…
Read Full BioSources
Rajpal S, Tong MS, Borchers J, et al. Cardiovascular magnetic resonance findings in competitive athletes recovering from COVID-19 infection. JAMA Cardiol. 2020;Epub ahead of print.
Disclosures
- Rajpal and Puntmann report having no conflicts of interest.
- Kim reports receiving compensation for his role as cardiologist for the Atlanta Falcons.
Comments