Colchicine Lowers CVD Risk No Matter When Past ACS Occurred: LoDoCo2
Even if stable patients had an ACS more than 7 years ago, they can still benefit from adding colchicine to medical therapy.


Investigators report that regardless of when the event happened—in the last 6 to 24 months or more than 7 years ago—colchicine effectively lowered the risk of major cardiovascular events compared with placebo in all patients.
“Our analyses of the LoDoCo2 trial show that patients with a history of very remote ACS remain at high risk of recurrent major adverse cardiovascular events, and that the efficacy of colchicine in patients with chronic coronary disease is independent of prior ACS status, producing consistent benefits irrespective of time since the most recent ACS event,” Tjerk S. J. Opstal, MD (Radboud University Medical Center, Nijmegen, the Netherlands), and colleagues write in their paper published online August 23, 2021, in the Journal of the American College of Cardiology.
To TCTMD, senior investigator Jan H. Cornel, MD, PhD (Radboud University Medical Center), said the post hoc analysis shines a light on the enduring risk seen even in patients with very stable CAD. For example, there were 4.3 major CVD events per 100 person-years in those with a very remote ACS. In contrast, there 3.4 and 3.3 major events per 100 person-years in those without a prior ACS and those with a much more recent ACS (within 6-24 months).
“The risk still persists in patients treated according to our guidelines,” said Cornel. “That includes high-dose statins, ACE inhibitors, aspirin, beta-blockers—they were very well treated. We saw a large reduction not only in hard endpoints, like stroke and myocardial infarction, but also in revascularization. Regardless of your history of having ACS or not, regardless of the timing of the ACS, colchicine seems to work in this all-comer population.”
Timing of Prior ACS
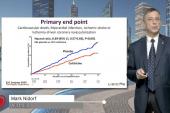
The LoDoCo2 trial, which was presented last year at the European Society of Cardiology (ESC) Congress and published at the time in the New England Journal of Medicine, included 5,522 patients with chronic CAD who had been clinically stable for at least 6 months. Over a median follow-up of 28.6 months, the addition of colchicine 0.5 mg to optimal medical therapy significantly reduced the risk of the primary endpoint, a composite that included cardiovascular death, spontaneous MI, ischemic stroke, or ischemia-driven coronary revascularization, when compared with placebo.
In total, 16% of the randomized patients had no prior ACS, 27% had a recent ACS (within 6-24 months), 29% had a remote ACS (within 2 to 7 years), and 29% of patients had a very remote ACS (more than 7 years). For those with a prior acute event, the median time from the ACS to randomization was 4 years.
In the adjusted and unadjusted analyses, there was no significant difference in the incidence of the primary endpoint among patients with and without a prior ACS who were treated with colchicine (P = 0.43 for interaction). Additionally, the reduction in risk observed with colchicine was consistent in those with a recent, remote, and very remote ACS (P = 0.59 for interaction).
Risk Reduction With Colchicine in Patients Stratified by ACS Timing
|
|
HR (95% CI) |
|
Prior ACS |
0.81 (0.52-1.27) |
|
Recent ACS (6-24 Months) |
0.75 (0.51-1.10) |
|
Remote ACS (2-7 Years) |
0.55 (0.37-0.82) |
|
Very Remote ACS (> 7 Years) |
0.70 (0.51-0.96) |
Cornel said that very stable CAD is still associated with low-grade inflammation, a state that colchicine would be expected to address given the drug’s anti-inflammatory properties. The results from this latest analysis suggest that the benefits of colchicine would be consistent if started “months or even years after ACS,” say investigators. At present, colchicine is not commonly given to patients with chronic or acute coronary syndromes, said Cornel, but he expects that to change.
“It’s my expectation that with two randomized, placebo-controlled trials—COLCOT and LoDoCo2—there’ll be some shift in the guidelines,” said Cornel, noting that CVD Prevention guidelines will be presented in the next couple of days at the 2021 ESC Congress. Also at this week’s ESC meeting, researchers shared data from the COVERT-MI trial, published in Circulation, showing no reduction in myocardial injury for STEMI patients given colchicine at the time of reperfusion then for 5 days thereafter.
In an editorial, Jean-Claude Tardif, MD, and Guillaume Marquis-Gravel, MD (Montreal Heart Institute, Canada), say the LoDoCo2 analysis extends the evidence supporting the safety and efficacy of colchicine to lower the risk of vascular events in patients with a recent MI, as in the COLCOT trial, and those with chronic CAD, as in LoDoCo2. “These data support the evolving story showing benefits of colchicine therapy in patients with coronary artery disease, including those presenting with acute coronary syndromes,” they write.
Cornel noted that doctors have been reluctant to prescribe colchicine because of concerns about gastrointestinal intolerance and other side effects, but that was mainly because of the historically large doses required to treat pain accompanying flare-ups of gout. The randomized trials, as well as other data, have demonstrated that low-dose colchicine is safe, said Cornel. In fact, he along with lead author Philip Robinson, MBChB, PhD (University of Queensland School of Clinical Medicine, Herston, Australia), outline the safety of low-dose colchicine for the treatment of gout and CVD in a recent consensus statement published in the American Journal of Medicine last week.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Opstal TSJ, Fiolet ATL, van Broekhoven A, et al. Colchicine in patients with chronic coronary disease in relation to prior acute coronary syndrome. J Am Coll Cardiol. 2021;78:859-866.
Tardif J-C, Marquis-Gravel G. Low-dose colchicine for the management of coronary artery disease. J Am Coll Cardiol. 2021;78:867-869.
Disclosures
- Opstal reports no relevant conflicts of interest.
- Cornel reports serving on the advisory board for Amgen and AstraZeneca.
- Tardif reports grant support from Amarin, AstraZeneca, Ceapro, DalCor Pharmaceuticals, Esperion, Ionis, Novartis, Pfizer, RegenXBio, and Sanofi; honoraria from AstraZeneca, DalCor Pharmaceuticals, HLS Pharmaceuticals, Pendopharm, and Sanofi; minor equity interest in DalCor Pharmaceuticals; and is included on submitted patents for pharmacogenomics-guided CETP inhibition.
Related News


Comments