DCB Outdo Noncompliant Balloons in Simple Bifurcation Side Branches: DCB-BIF
Why DCBs reduced MIs but had no impact on TLR isn’t clear—studies in more-complex lesions could enlighten.

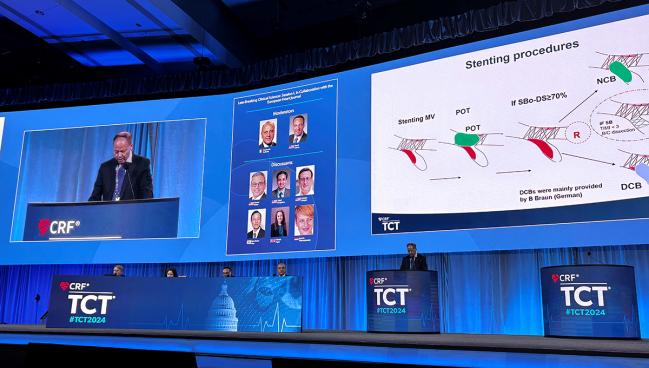
WASHINGTON, DC—For patients with simple, true coronary bifurcations treated with a provisional-stenting strategy, use of a drug-coated balloon (DCB) rather than a noncompliant balloon (NCB) in the pinched side branch (SB) produces better 1-year outcomes, according to results from the DCB-BIF randomized trial.
Most of the difference in overall MACE was tied to a reduction in target-vessel MI, though these events occurred early and didn’t necessitate revascularization, Shao-Liang Chen, MD (Nanjing First Hospital, Nanjing Medical University, China), reported here at TCT 2024.
Led by first authors Xiaofei Gao, MD, Nailiang Tian, MD, and Jing Kan, MD (all from Nanjing First Hospital, Nanjing Medical University), the study was simultaneously published in the Journal of the American College of Cardiology. The DCB-BIF investigators point out that the preferred approach to straightforward bifurcations < 10 mm is provisional stenting, wherein a stent is implanted in the main vessel but not necessarily in the side branch.
“Side-branch stenting is often required during provisional stenting, leading to suboptimal results,” Chen told TCT attendees. For several reasons, DCB have “emerged as an attractive strategy” for treating the side branch, he added. “However, the benefit of DCB for coronary bifurcations remains unclear.”
Noncompliant balloons can be used, but these can result in dissection or abrupt occlusion, the researchers note. Stents in the side branch, on the other hand, can develop restenosis that leads to stent thrombosis and repeat revascularization, they say. “Therefore, the concept of ‘nothing left’ after SB intervention using a drug-coated balloon is appealing to most interventional cardiologists.”
The paclitaxel on the DCB’s surface offers the added bonus of reducing intimal hyperplasia, potentially attenuating restenosis and reducing cell differentiation.
Nicola Ryan, MB, BCh, BAO (Aberdeen Royal Infirmary, Scotland), the discussant for DCB-BIF in the late-breaking session at the meeting, said the study—the first randomized trial to compare DCB versus NCB for bifurcation lesions—is important and clinically relevant.
She highlighted a number of uncertainties, though, among them that the researchers did not specify which type of DCBs they used. “As we all know, drug-coated balloons are not equal and we cannot consider a class effect within them, as there are differences in the balloon design, the drug dosing, the drug delivery, and the pharmacokinetics amongst the drugs,” said Ryan.
Still, she concluded, the results do hint that DCB may be a beneficial strategy in the side branch of true, noncomplex bifurcation lesions.
Lower MACE Rate at 1 Year
For the DCB-BIF trial, the researchers enrolled 784 patients (median age 65 years; 76.7% men) with true, simple coronary bifurcation lesions who underwent main-vessel stenting and then were found to still have a severely compromised SB (residual stenosis ≥ 70%). The study took place at 22 centers in China, Indonesia, Italy, and Korea over a 3-year period, with participants randomized to receive either DCB or NCB intervention in the pinched SB.
Nearly four in 10 had type 2 diabetes. Most (61.1%) presented with unstable angina, followed by NSTEMI (24.5%), stable angina (6.8%), STEMI (5.7%), and silent myocardial ischemia (2.2%). Three-quarters of patients had Medina 1,1,1 bifurcation lesions, and two-thirds had multivessel disease. For 67.9%, the bifurcations were located in the left anterior descending artery, while 15.2% had this anatomy localized at the distal left main.
PCI was done almost exclusively using a transradial approach with a 6-Fr guiding catheter. IVUS guidance was used in 22.6% of patients and OCT guidance in 4.7%. After stenting the main vessel and ballooning the SB, operators performed kissing-balloon inflation in 96.9% overall (94.9% with DCB vs 98.9% with NCB; P < 0.001) and used a repeat proximal optimization technique in 83.9%.
Fully 100% of the NCB group and 97.4% of the DCB group received their randomly assigned treatment, with 1% of the NCB group also receiving a DCB. Around 3% in both groups crossed over to a two-stent approach.
At 1-year follow-up, Kaplan-Meier estimates showed a reduction in the primary endpoint of MACE (cardiac death, target-vessel MI, or clinically driven TLR) for the DCB group compared with the NCB group (7.2% vs 12.5%; adjusted HR 0.56; 95% CI 0.35-0.88).
The difference was driven mainly by fewer target-vessel MIs, a category that included both periprocedural MIs within 48 hours and spontaneous MIs after 48 hours, among DCB-treated patients (5.6% vs 10.9%; adjusted HR 0.50; 95% CI 0.30-0.84). Looked at separately, there was a significant reduction in spontaneous MI (1.0% vs 3.6%; adjusted HR 0.27; 95% CI 0.09-0.81) but not periprocedural MI (4.6% vs 7.4%; adjusted risk difference -2.8%; 95% CI -6.23% to 0.59%).
Rates of procedural success, crossover to a two-stent approach, all-cause death, revascularization, and stent thrombosis did not differ between the DCB and NCB groups.
The number needed to treat was 18.9 to prevent MACE and 38.5 to prevent spontaneous MI. While the advantage of DCB did not differ in various subgroup analyses, there did appear to be “more profound” benefits in patients ages 65 and older, those whose bifurcations were not in the left main, and in cases without intravascular imaging guidance, Chen reported.
Looking at more complex lesions where the stakes are higher might produce [clearer] results. Celina Yong
Celina Yong, MD (Stanford University School of Medicine, CA), who co-wrote an editorial accompanying the paper, told TCTMD that the DCB-BIF data are promising but also counterintuitive—in particular, the lack of difference in target lesion revascularization begs the question of why the MIs that occurred don’t appear to have been acted upon.
“At face value, the results of the study suggest DCBs are a great option for a simple side-branch bifurcation, but I think when you really dive deep into the specifics of what they found, it’s not that clear,” she commented.
Yong pointed out that the Kaplan-Meier curves show the MIs are happening very early, with the follow-up angiograms occurring later. “To me, that suggests that the investigators weren’t looking, because either the lesion itself they thought was not significant enough [to need it] or they knew it was going to be hard to treat if they went back in there,” she explained, adding that altogether this makes it hard to interpret the observed benefit with DCBs.
Jeffrey W. Moses, MD (NewYork-Presbyterian/Columbia University Medical Center, New York, NY), in a press conference ahead of the session, also seemed perplexed by the data. “This is a very interesting study and frankly very confusing. Have you characterized the patients that had the MIs but didn’t have revascularization? It’s kind of unusual. I just hope we’re not going to have a [glycoprotein] IIb/IIIa situation where we’re chasing biomarkers and not clinical events,” he observed.
Chen agreed this is a key question, suggesting that the discrepancy may have arisen because their study population had simple coronary bifurcations as well as “pretty low” revascularization rates within the 1-year follow-up duration. “I think it would be very difficult to get a significant reduction in the revascularization,” said Chen, adding that a study of more-complex bifurcations might be able to detect a difference.
Yong, in the press briefing, said this might be a way forward: “Looking at more complex lesions where the stakes are higher might produce [clearer] results.”

Caitlin E. Cox is Executive Editor of TCTMD and Associate Director, Editorial Content at the Cardiovascular Research Foundation. She produces the…
Read Full BioSources
Gao X, Tian N, Kan J, et al. Drug-coated balloon angioplasty of the side branch during provisional stenting: the multicenter randomized DCB-BIF trial. JACC. 2024;Epub ahead of print.
Ali Z, Yong CM. Drug-coated balloons to keep interventions of the side branch simple (KISS): KISS or be KISS’D. JACC. 2024;Epub ahead of print.
Disclosures
- DCB-BIF was funded by the National Key Research and Development Plan, the Chinese Society of Cardiology, the National Natural Scientific Foundation of China, and the Jiangsu Provincial and Nanjing Municipal Clinical Trial Project. It was jointly supplied by B. Braun Medical, Shenqi Medical, Yinyi Medical, Yingsheng Medical, and Kaidenuo Medical.
- The researchers and Yong report no relevant conflicts of interest.
Related News



Comments