Good Results but Small Numbers With JenaValve Trilogy in Severe AR
Treatments are limited for surgery-ineligible patients with severe AR, but this particular TAVI system is raising hopes.

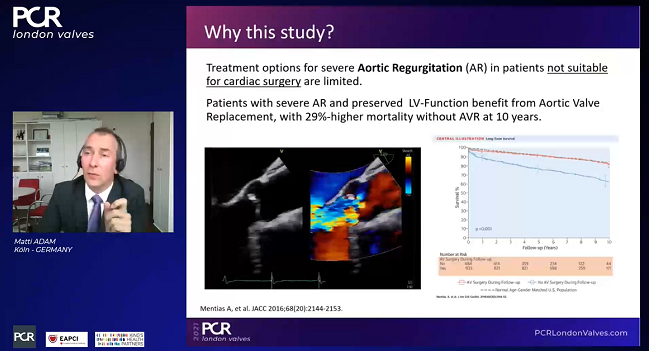
Transcatheter aortic valve implantation to treat aortic regurgitation (AR) appears to be a relatively safe and effective option in high-risk patients ineligible for surgery, according to a small series presented this week.
“We had quite good results,” Adam told TCTMD. “The procedure was successful in nine out of 10 patients, and we decreased aortic regurgitation significantly. We also saw that the patients improved in terms of NYHA class. The JenaValve might be a promising device for these patients.”
In the US, there is no TAVI system approved for the treatment of surgery-ineligible patients with severe AR, but the JenaValve Trilogy device earned CE Mark approval in Europe this past May for such patients. It is also approved in Europe for the treatment of aortic stenosis.
Surgical aortic valve replacement for severe, symptomatic AR remains the gold standard in both the American and European clinical guidelines for valvular disease. One concern with TAVI is the risk of valve migration and paravalvular leak. The latest guidelines from the European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) state that TAVI “may be considered in experienced centers” only for selected patients who are ineligible for surgery.
“Aortic regurgitation, in terms of the anatomy of the valve, is a different animal than aortic stenosis,” said Adam. “Calcification of the cusps is often absent, there might be dilation of the aortic root or of the ascending aorta. When we treat these patients with the devices we have available now, the results aren’t as good as they would be if we were treating someone with aortic stenosis. What could make a difference—and we need more data of course—is the design of the valve.”
To TCTMD, Firas Zahr, MD (Oregon Health and Science University, Portland), who is involved in the ALIGN-AR trial testing the Trilogy TAVI system in high-surgical-risk patients with severe AR, said they frequently encounter these types of patients, leaving physicians in a quandary.
"Unfortunately, many of these patients remain symptomatic despite being on optimal medical therapy, and there is a big knowledge and technology gap in treating these patients,” he said.
Currently available commercial TAVI devices are not ideal for treating patients with severe AR due to the absence of calcium to anchor the devices, and “although there are some case reports of successful implants, the results are not reproduceable and are limited to only a few highly selected patients with severe aortic insufficiency,” said Zahr.
What could make a difference—and we need more data of course—is the design of the valve. Matti Adam
Andrew Goldsweig, MD, MS (University of Nebraska Medical Center, Omaha), said that high-risk aortic valve surgery will often be performed in severe, symptomatic AR patients, but if it absolutely can’t be done, implantation of a left ventricular assist device, off-label TAVI, or palliative medical therapy are the three options. He noted that patients turned down for surgery are frequently older and have significant renal disease, which can result in aortic valve calcification.
“If adequate calcium is present to deploy a TAVR valve, off-label TAVR is possible for AR, and these patients do very well,” Goldsweig told TCTMD. “However, without adequate valvular calcium, TAVR is not possible with our currently available valve technologies. If left ventricular dilation and systolic failure are the reason that [surgery] is not preferred, then [a] destination LVAD may be reasonable. Of course, despite all of the advances in structural heart disease, some patients truly have no options other than palliative medical therapy.”
Technology Promising
At the moment, the JenaValve Trilogy device is one hopeful option for surgery-ineligible patients undergoing TAVI, said Adam. The transfemoral system includes three locators that allow operators to clip the aortic leaflets and implant the prosthesis in a manner that ensures commissural alignment. The use of locators to clip the aortic cusps also allows the device to be fixed and sealed in place once it opens, which protects against valve migration and paravalvular leak.
In their series, all 10 patients were deemed ineligible for surgical aortic valve replacement (median STS score 7.6%). Seven patients presented with severe AR and three had moderate AR, but all patients had NYHA class III/IV symptoms. The mean annulus size was 26.4 mm, ranging from 23.9 to 29.4 mm. The reasons for surgical turndown were numerous, including the presence of significant comorbidities and a preexisting LVAD in two patients.
TAVI was successful in all but one patient, a valve-in-valve patient who required bailout with a different TAVI device. No moderate/severe AR was observed at discharge. In total, seven of the 10 patients had a functional improvement to NYHA class I/II symptoms, which Adam deemed “a significant improvement in the clinical presentation of our patients.”
Despite all of the advances in structural heart disease, some patients truly have no options other than palliative medical therapy. Andrew Goldsweig
Further studies are needed to prove the safety and efficacy of TAVI with JenaValve in patients with AR, said Adam, stressing this would include lower-risk patients than in their compassionate-use series. In August, the US Food and Drug Administration allowed the manufacturer to launch the investigational device exemption (IDE) ALIGN-AR study where investigators plan to treat 180 high-surgical-risk patients with severe AR and NYHA class II or greater symptoms with the JenaValve Trilogy.
Both Zahr and Goldsweig are eagerly anticipating the results from ALIGN-AR. Goldsweig noted that device does not exert significant pressure on the septum in the process of anchoring, and said he suspects that pacemaker implantation rates should be low. However, at the moment, data are really sparse. There are 1-year outcomes from the JUPITER registry of 30 patients with AR treated with the transapical JenaValve system, but the data is very limited with the transfemoral device, he noted.
Moderate-to-severe AR occurs more frequently than one would expect, said Adam. In the Framingham Heart Study, the prevalence of moderate-to-severe AR was roughly 1% in patients 70 years or younger, but approximately 2% in those older than 70 years. “It’s a bad prognosis,” said Adam. “Once they get symptomatic with AR, it’s not good.”
“We also know that SAVR can improve prognosis significantly in these patients,” he said. “But in a recent analysis, only 25% of patients with severe symptomatic AR were treated with SAVR within the first year. The untreated patients were more likely to be older and had worse left ventricular function. So maybe improved interventional strategies like a dedicated TAVI device could help to get these higher-risk patients the treatment they need.”

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Adam M, Wieneman H, Kodali S, et al. First clinical results of the JenaValve TAVI system in patients with aortic regurgitation. Presented at: London Valves 2021. November 24, 2021.
Disclosures
- Adam reports grant and research support from Medtronic and honoraria/consulting fees from Boston Scientific, Edwards Lifesciences, and Medtronic.
- Zahr reports receiving institutional grant support from Edwards Lifesciences and Medtronic.
- Goldsweig reports grant support from the National Institute of General Medical Sciences and the UNMC Center for Heart and Vascular Research.
Related News


Comments